Carrying out equality based impact assessments
advertisement

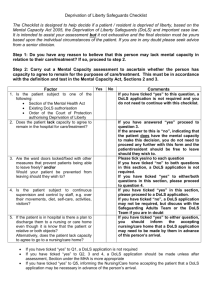
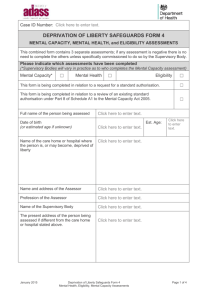
Derbyshire County Council Equality Impact Assessment Record Form 2010 Department Adult Care Service Area Responsible Safeguarding Chair of Assessment Group Sue Pearson Title of Policy/ Service/ Function Mental Capacity Act 2005 Deprivation of Liberty Safeguards Stage 1. Prioritising what to impact assess 1.1 Why has this policy, service or function been chosen? The Mental Health Act 2007 introduced the Deprivation of Liberty Safeguards (DOLS) as an amendment to the Mental Capacity Act 2005 (MCA). Any person in hospital or a registered care home that lacks capacity must be assessed in accordance with the Deprivation of Liberty Safeguards’ Code of Practice to legally deprive them of their liberty. The safeguards are intended to close the ‘Bournewood Gap’ identified by the European Court of Human Rights in order to provide protection and a legal framework for people who need to be deprived of their liberty, and where it is not appropriate to do so under the regime contained within the Mental Health Act 1983 and as amended by the Mental Health Act 2007. From April 1st. 2009 under the Mental Capacity Act, Derbyshire County Council acquired the responsibility of a Supervisory Body. It is required to have in place a policy and procedures, processes including governance, identified assessor roles and a knowledgeable workforce in order to meet its legal responsibilities. In addition to being a supervisory body, Derbyshire County Council has a role in supporting the Managing Authorities. It must also support the medical workforce working as Mental Health Assessors (MHA), the group of Best Interests Assessors (BIA), the Paid Representatives, and the IMCA (Independent Mental Capacity Advocacy) Service. This Equality Impact Assessment (EIA) is part of this governance process in that it seeks to identify potential differential or negative outcomes for people from different communities and put in place an -1- action plan to address these. The EIA is a systematic way of finding out whether DOLS affects all groups equally. It should address real or potential inequalities resulting from policy and practice, and will help identify how to better meet the needs of these diverse groups. This information is also required by the Department of Health (DH) on a quarterly basis. In addition this EIA is being undertaken as part of an ongoing programme to ensure that the authority’s policy, procedures, services and functions recognise diversity and promote inclusion. 1.2 Why does the policy, service or function exist/ what is its purpose? Who should benefit? The Deprivation of Liberty Safeguards’ aim is to ensure that an adult is not deprived of their liberty unless stringent processes as laid down in law have been followed. The new regime is intended to protect those who lack capacity, who may not dissent to or resist their care, and who need or may need to be deprived of their liberty in hospitals or care homes. This is whether placed under public or private arrangements for their own safety, and in their best interests for the purposes of their care or treatment. The care home or hospital providing their care, however, has what amounts to full control over their freedom to act. The safeguards do not cover people detained under the Mental Health Act as they already have the benefit of legal safeguards. The legislation requires the care home or hospital, the ‘Managing Authority’, to seek authorisation from the relevant ‘Supervisory Body’: (Local Authority or Primary Care Trust (PCT)) and contains detailed requirements about when and how deprivation of liberty may be authorised. It provides for a six-part assessment process that must be undertaken before deprivation of liberty may be authorised and detailed arrangements for renewing and challenging the authorisation of deprivation of liberty. Derbyshire County Council has developed detailed clear referral and assessment pathways within legal timeframes. All requests for Deprivation of Liberty Safeguards authorisations are considered by the Local Authority as the Supervisory Body, and are approved at a senior management level. All referrals for requests are treated equitably and all assessments for a deprivation of liberty authorisation are scrutinised. The assessment process is designed to ensure that where a request for a deprivation of liberty has been refused, appropriate actions are taken to ensure the person is receiving their care or support in the least restrictive and most person-centred way. Similarly, where a deprivation of liberty authorisation is approved, practice guidance ensures that the authorisation is subject to rigorous ongoing scrutiny and review in -2- accordance with the Code of Practice. The Code of Practice clearly references the importance of recognising different cultures and this is reflected in the Local Policy and Procedures. The desired outcome is to ensure that the rights of any adult lacking in capacity aged 18 and over, as laid down in accordance with the Human Rights Act 1998 and the Mental Capacity Act 2005, are upheld. This is intended to ensure that a vulnerable person’s needs are met in a person centred way, in the least restrictive setting, whether a hospital or care home setting and is compliant with the Mental Capacity Act 2005. Stage 2. Pulling an assessment team together Name Sue Pearson (Chair) Tracy Hutton Fiona Lloyd Rob Gordon Martin Hammond-Hallam James Gough Denise Bate Joan Webster Dr. Simon Nissenbaum Prof. Reinhard Heun Dr. Ivan Bakaltchev Sarah Bendikas Stage 3. Area of expertise/ role DOLS Service Manager (Derbyshire County Council, Derbyshire County PCT) Best Interests Assessor Best Interests Assessor Best Interests Assessor Best Interests Assessor Best Interests Assessor Paid Representative Paid Representative Mental Health Assessor Mental Health Assessor Mental Health Assessor Derbyshire Independent Mental Capacity Advocate Scoping of the assessment / identifying likely issues This EIA will seek to identify whether guidance and related information and training on DOLS is sufficient to meet the needs of all sections of the community particularly those people from ReGARDS (Religion, Gender, Age, Race, Disability, Sexuality) communities. In doing so it focuses on: Information and guidance for staff working in social care, either within the authority or across other disciplines, including professionals working in health. This will also include that for staff in care homes supporting residents, whether local authority or private, voluntary and independent sector. -3- Information that is available to members people experiencing DOLS, their carers, families and the wider public Likely issues identified relevant to the equality impact assessment: -Quality and relevance of awareness- raising sessions through training and education of all staff groups, including local authority and private registered care providers -Problems with communication between the different organisations and understanding of the processes and the legal timescales for dealing with the referrals. Public facing information includes Easy Read versions of booklets and information, as well as availability of information in other languages if required. Training is being rolled out on an ongoing basis to staff and professional groups, but it is clear additional training and support is required. Feedback from staff through meetings and briefing sessions has clearly identified a lack of understanding of the process of DOLS referrals despite having received training on it. It has also been identified after talking to Service Users and their families that there are real difficulties experienced in understanding the process of the authorisations and why it is taking place. There is a perception from care home managers and staff that DOLS is viewed as negative and to be avoided. It is not viewed as linking to the personalisation agenda and being part of the process of enabling adults without capacity to have greater choice, planning and control of their care. A further likely issue identified is around unlawful deprivation of liberty. This may occur in institutions where there is an embedded culture of delivering care and practice, which may not consider an individual’s rights. Stage 4. Pulling together all the information Name of source Statistical information from various sources including census, Joint strategic needs assessment Audit several homes which have applied for an authorisation Feedback from Best Interests Assessors Feedback from Mental Health Assessors Feedback from Paid Reason for using Profile of county, population, communities and projections of need Provides focused information on the experience and highlights difficulties and areas where more support and information required Professional perspective on the process for an application Professional perspective on the process for an application Professional perspective on the -4- Representatives Feedback from IMCA Service Feedback from carers/families Feedback from CQC Inspectors Stage 5. 5.1 process for an application Professional perspective on the process for an application Consultation on the impact/experience of the referral process Professional perspective on the process for an application Assessing the impact or effects What does customer feedback, complaints, and discussions with stakeholder groups tell you about your service, policy and function, including which aspects are seen as negative, inaccessible, unhelpful, difficult to use etc? Feedback of the type of referrals so far illustrate that it is predominantly older adults who are being referred under DOLS. There have been no referrals so far from different ethnic groups or identifying sexual orientation. There are more female older adults referred, and a higher number of males with a learning difficulty. Feedback from service user groups, healthcare professionals and staff indicates a widespread lack of awareness and understanding of the DOLS legislation and the legal timeframe for applications and assessments. This has clearly identified issues around training and accessing training, particularly for the private, voluntary and independent sector, and the ensuing understanding of the process. This feedback has highlighted the poor level of understanding of the Mental Capacity Act and decision making, and that consideration of the MCA around capacity and best interests are not routinely embedded in all aspects of care of vulnerable adults lacking in capacity. There is a lack of understanding on how to complete the forms and information provided by the care homes indicates care plans are not updated and care may not be person-centred. Professional staff, in order to be compliant with the Mental Capacity Act 2005, should have a general awareness of care planning to reduce restraint and avoid situations where people are deprived of their liberty. This will also assist them to understand DOLS and be able to identify when they will need to seek an authorisation. Staff will be able to direct care planning so as to avoid deprivation, and where this is not possible, request an authorisation. -5- The lack of awareness around DOLS has meant that few unauthorised (unlawful) deprivation of liberty has been identified. This means there is potentially a large group of vulnerable people who are not accessing the safeguards. A Derbyshire IMCA who made a 3rd. party referral under DOLS for a care home has recently highlighted this. Feedback from the IMCA identified a lack of training and awareness around DOLS as an issue within this care home. The DOLS Code of Practice clearly references the importance of recognising different cultures and this is reflected in our Policy & Procedures. This will enable the Local Authority to identify and highlight any discrimination. There are significant human/civil rights issues under DOLS, with the potential for legal challenge and also inequalities, so the monitoring and governance of the safeguards are key. The DOLS Team, Best Interests Assessors and Training Team will work to develop staff confidence in the process of referring under DOLS. 5.2 What does your information tell you about the effects of the policy, service or function on the lives of different groups or communities? Is any of this negative or unwanted? Groups Older Adults Effects identified from data/ information Older Adults represent the largest single source for referrals; these are primarily related to perception of risk. Dementia, which is more prevalent in this age group, is the major reason for lack of capacity. Compliance with the implementation of the safeguards and the authorisations remains variable, and corresponds to lack of training and awareness in care providers. Sometimes relevant statutory duties with a proper regard for Human Rights may not take into account the impact of lifestyle choice issues on group living. Where the safeguards are implemented correctly, the effect on an individual’s care are very positive and reflect Human Rights and gives this group of disadvantaged people protections that have previously been lacking. -6- Race/ethnicity Gender Sexual orientation Disabled people Younger People However, addressing the Human Rights of adults who are vulnerable through frailty or ill health is a key responsibility of all statutory agencies with a public protection responsibility. Evidence suggests that black and minority ethnic communities are less likely to access statutory services. However, lack of training and awareness in care providers may contribute to this. There are currently few referrals under DOLS and little information to identify whether the safeguards are being applied differently in relation to different racial or ethnic groups. A large proportion of DOLS referrals are for people with dementia, and data submitted to DH indicates a higher ratio of older females being subject to the safeguards. Data also indicates a higher number of males with learning difficulty. There is currently no feedback to highlight the impact of DOLS. However, lack of training and awareness in care providers may contribute to this. There are an increasing number of referrals for this client group, with a higher proportion of younger males being referred. There is a key responsibility of all statutory agencies with a public protection responsibility to address their Human Rights and to take into account and consider the impact on group living. Through DOLS, there is a new focus on their Human Rights and the lawfulness of the arrangements made for their care. These adults are vulnerable through their disability, and many have lived in institutions for most of their lives. The safeguards apply to anyone aged 18 and over. Referrals in this age group tend to be for young people with a learning difficulty who receive institutionalised care. Referrals relate to perception of risk for the individual, other service users and staff. Compliance with the implementation of the safeguards and the authorisations remains variable, and corresponds to lack of training and awareness in care providers. -7- Stage 6. Ways of reducing or removing unwanted effects What small steps could be taken to achieve improvements? Please outline the main things that need to be altered to reduce any illegal, negative and unwanted impact. Increase awareness/knowledge of healthcare professionals and LA staff - evaluate existing training of both MCA and DOLS and its effectiveness on good practice. Additional training may need to be provided, especially to homes/institutions with a culture of restrictive practice. The 3 new fulltime BIA Lead Practitioner posts will be instrumental in offering additional support and information to such homes. Feed information from the DH audit of MCA and DOLS starting in April 2010 from care homes in the county; this will help to identify homes with specific training needs. This information can be used to decide whether disparities between groups amount to adverse impact on some groups or unlawful discrimination. Derbyshire County Council to undertake an audit of all the care homes in Derbyshire around understanding/implementing the Mental Capacity Act and DOLS. This audit, which starts in April 2010, will serve to highlight and assess the impact of DOLS on our care homes and will provide information and feedback as part of this EIA. The audit will help illustrate the numbers of possible referrals for the ReGARDS group as this is currently an area which is under represented. Consult interested parties, service users and members of the public on awareness of DOLS: this could be achieved formally through the DH audit or informal approaches such as service user representatives, focus groups or questionnaires. Information systems- information from the DOLS database is currently being transferred to Framework i to ensure a better integration of service user information and a more efficient and streamlined approach to storage of service user information. This will be made available to other healthcare professionals involved in DOLS such as BIAs from the PCT. DOLS information also to be developed and updated on Derbyshire Intranet (DNet) with consideration being given to a frequently asked questions ‘FAQs’ web page which could offer advice -8- and support through information sharing. Ensure existing materials and information from the DH and regional forums are accessible and available and appropriately distributed. This information must be made available in different formats and languages if required. Stage 7. Finding out whether your assessment has identified what people think needs changing. This assessment and the resulting action plan has been developed and agreed by the DOLS assessment team. The group who will report on actions taken to senior management will monitor the implementation of the actions arising from the EIA. -9- Stages 8 and 9 - Action planning, target setting and monitoring TARGETS / SUCCESS CRITERIA LEAD RESP PARTNER INPUT RESOURCES PERFORMANCE INDICATORS/ MILESTONES Project lead Simon Stevens (MCA Lead), BIA Lead Practitioners Training events including a DOLS conference in May 2010 Increase in appropriate DOLS referrals and staff confidence Improved communication between the different partners, including PCT, private, voluntary and independent sector, commissioners and providers DOLS assessm ent team Health/PCT Framework i DNet Training and information materials widely available Increase in appropriate DOLS referrals and staff confidence around the legislation, increased awareness in minority groups Address lack of awareness of DOLS with interested parties such as service users, their families, members of the public Project lead & BIA Lead Practition ers DOLS Assessment Team, care home managers Focus groups, Positive feedback representatives of care homes , from DH audit questionnaires ACTION Liaise with the Training Team to review existing training and its effectiveness to be well understood and embedded into practice - 10 - QUALITY ASSURANCE PERFORMANCE INDICATORS/ MILESTONES LEAD RESP PARTNER INPUT To streamline information systems working in partnership with other resources such as Frameworki DOLS Team DCC IT team Measurement of ease of access to service user information from secure database; information more easily accessible to healthcare professionals involved in DOLS referrals and care DOLS information on DNet to be kept updated Project lead BIA Lead Practitioners Increase in confidence and understanding of DOLS & referral process Ensure provision of clear information available in poster/leaflet form and available in translated versions Project lead BIA Lead Practitioners Increase in confidence and understanding of DOLS & referral process ACTION - 11 - RESOURCES QUALITY ASSURANCE Step 10. Have your main actions been added to the relevant business or service plan(s)? Please indicate below which actions to which plans Action planned Liaise with the Training Team to review existing training and its effectiveness to be well understood and embedded into practice Joint multi-agency group to be set up to look at improved communication between the different partners, including PCT, private, voluntary and independent sector, commissioners and providers Address lack of awareness of DOLS with interested parties such as service users, their families, members of the public To streamline information systems working in partnership with other resources such as Framework i DOLS information on DNet to be kept updated Ensure provision of clear information available in poster/leaflet form and available in translated versions Business / Service Plan Training Business Plan How will performance be tracked and reported? Evaluation arrangements in place with lead practitioners MCA DOLS 1st meeting in September 2010 Terms of Reference Information advocacy and Advice work stream and plans Evaluation of Audit information Information Management Live in Framework I on 02.08.10 Communications DOLS information up to date and will be included in all routine updates reported through Information Team Communications DOLS information is current and up to date in any DCC adult care leaflets that reference it. Reported through information Team - 12 - Step 11. Publishing your assessment Please indicate below:Your assessment has been signed off for publishing by Your assessment was published on Medium/ location Date Signed Andrew Milroy Date 27th July 2010 Added to DCC website - 13 -