Notes for Lectures on the Concepts of Transference
advertisement

12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 1 Notes for Lectures on the Concepts of Transference and Countertransference in Psychoanalysis, Psychoanalytic Group Psychotherapy and Group Analysis © Earl Hopper, Ph.D. This paper has benefited from the critical comments of several colleagues who I will be pleased to acknowledge when I publish a later version of it. 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 2 The purpose of this monograph is twofold: to summarise our knowledge of the concepts of transference and countertransference; and to consider some of the most important steps in the development of our thinking about the processes to which these concepts refer. Key books and articles are cited. I will also indicate some of my own doubts and confusions about how the concepts of transference and countertransference are used both in the literature and in clinical work. This monograph is intended to be a kind of extended entry in a ‘dictionary’ of the main concepts in our work. Space does not permit detailed clinical and empirical examples. Analysts show great diversity in how they use the concepts of transference and countertransference, especially in their clinical work. Some sense of this diversity, both for good and for ill, can be gleaned from Hamilton’s (1996) study of ‘psychoanalytical cultures’. Clearly, the concepts of transference and countertransference can only be understood in their theoretical and meta-theoretical context. For example, using these concepts implies that we believe that we are able to be both subject and object, and have sufficient ego-freedom to reflect on our experiences, identities and wishes, and to distinguish what we have been and what we are from what we wish to be. Nonetheless, it will not be possible here even to outline the general models of psychoanalysis and group analysis. They must be taken for granted, although in doing so more questions might be raised than answered. In Part I, I will discuss the concepts of transference and countertransference in psychoanalysis and psychoanalytical psychotherapy. In Part II, I will discuss these concepts in psychoanalytical group therapy and group analysis. In the Conclusion, I will focus on considerations that apply to both fields of study and clinical work. Part I TRANSFERENCE: THE WORK OF FREUD 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 3 The usage of the terms ‘transference’ and ‘countertransference’ has changed and developed as psychoanalysis has changed and developed. Thus, to understand the meaning of these terms it is necessary to take an historical perspective. As usual, this means starting with the work of Freud, recognising, of course, that like Darwin and others, Freud was both a genius and a child of his time, which in essence was the second half of the 19th Century. However, Freud wrote over many decades, and hypothesised several models of the mind and models of the treatment relationship (Laplanche and Pontalis, 1973), and his use of the concepts of transference and countertransference must be understood within the context of his own developing work. In the first instance, he used ‘transference’ to refer to a kind of intellectual contagion that takes place from one set of words and ideas to another. As such, it could produce confusion based on what might even be called ‘wrong thinking’ or ‘bad thinking’, in which a person uses a word or an idea which seems to the listener or reader to be out of the context assumed by the speaker. This usage of ‘transference’ very quickly gave way to an understanding of transference as ‘resistance’ to intellectual insight and understanding. Thus, Freud wrote about ‘transference resistance’. There were other forms of resistance, but transference resistance came to be of central importance, because it referred to something that was going on between patient and analyst such that the patient refused to understand the good thinking and interesting ideas offered by the analyst. In other words, as someone or another has said, Freud’s patients would just keep trying to turn things into emotional affairs, refusing to knuckle down and understand what Freud was talking about. In other words, these treatment failures were due to his patients being overly emotional. This understanding of transference as resistance to intellectual insight can be traced to the origins of psychoanalysis in hypnosis and hypnotherapy, which was used in order to enhance the influence of the hypnotist/doctor and his ideas in a way that would increase the likelihood that the resistances of the patient would be overcome. 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 4 The third and most important way in which Freud used ‘transference’ was to refer to a repetition of psychic reality in the treatment relationship. This idea has been modified several times, but it has remained central in the psychoanalytical perspective. Three main points are involved. The first is that transference concerns ‘psychic reality’ or ‘psychic experience’, not ‘historical reality’. The second is that psychic reality is governed by ‘psychic determinism’, or in other words, principles of causation apply to the human psyche. These principles of causation also govern the forces of ‘constitutional factors’, to be understood in terms of the sciences of inorganic and organic matter, as well as the forces of so-called ‘external’ factors, to be understood in terms of the social and psychological sciences, using these labels to convey a multitude of phenomena. We all exist in time and space in a particular way, and inevitably our perceptions will be influenced by who and what we have been and the experiences that we have had, which include the experiences of the body, mediated through the veils and tools of language and communication in general. The third point about transference as repetition of psychic reality within the treatment relationship is the recognition that it is in the nature of the human condition that we are always and necessarily caught in transferences in the most general sense of the term. Therefore, unless we locate (Bernfeld, 1929) the transference within the context of the treatment relationship, we are not saying anything very interesting. The repetition of psychic reality in the treatment relationship is a specific phenomenon with its own parameters, an understanding of which offers a tool for psychoanalytical work. The discovery of the transference and the emphasis on its interpretation in clinical work is the hallmark of psychoanalysis. For example, Freud argued that the analysis of the transference and the transference neurosis was the battleground of treatment. This is where the war against psychopathology would be won. This was a continuation of the idea that the transference was a resistance to insight offered by the analyst. Freud was always a kind of fight/flight leader, and this is the language that he used. The analyst would win the battle against 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 5 illness through the interpretation of the transference neurosis, provided that the patient could listen and hear. It is very important not to offer ‘transference cures’ or to collude with ‘flights into health’. Freud rejected the idea from the earlier hypnosis-phase of psychoanalysis that if a patient established a highly idealised and idealising relationship with the analyst who had magical powers, he would then get better, because this would not really be a proper analytical cure, and certainly would not be very long lasting. That is what happens in cults, but not in psychoanalysis. However, Freud acknowledged that transference cures occur within psychoanalysis, and that such cures can be very helpful. Freud distinguished between positive transference and negative transference, both of which required analysis. However, he also suggested that in a way patients were cured on the basis of their positive transferences, that is to say, their reproduction in the treatment relationship of their basic loving feelings based on loving experiences. The analyst who is perceived in these terms has the power to ‘cure’ or to ‘heal’. However, Freud remained somewhat unclear and uncertain as to the benefits that might accrue from the analysis of positive transferences. Freud indicated that drives, fantasies, conflicts and object relationships, in fact everything that goes on in the mind, is available for the transference. Many years later Melanie Klein (1952) referred to the ‘total situation’ of the patient, by which she meant all the contents of the mind in relationship to mother and father and even the family, not only during infancy but also during childhood. Thus, according to Freud and to Klein , the total situation of the patient is available for the transference. In sum, Freud started by: ‘…looking at what the patient brought into the treatment (and found) aspects of behaviour that at first he regarded as a technical obstacle; later saw that it was inevitable that the patient transferred into the relationship with the analyst old patterns of behaving and relating; then saw that this was actually helpful, and finally that it was a major tool in understanding and treatment’. (Joseph, 2003, p.147). As Anna Freud (19xx) explained: ‘By 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 6 transference we mean all those impulses…’ and defensive manoeuvres against them ‘…which are not newly created… but have their source in early – indeed the very earliest – object relations and are now merely revived under the influence of the repetition compulsion’ (p.118). TRANSFERENCE: DEVELOPMENTS An important turning point in British psychoanalysis occurred in 1937 when James Strachey, one of the Bloomsbury set and one of the first analysts in Britain, wrote ‘On the nature of the therapeutic action of psychoanalysis’. In the olden days, when I first trained, in the late 1960’s, we were obliged to start with Strachey’s article. It explained why psychoanalysis offered something that other forms of treatment did not, why psychoanalysis was the Heineken of psychotherapies, namely, that if you analysed/interpreted the transference you would be able to make a mutative interpretation, one that would bring about a structural change in the mind based on insight. This conviction was based on the assumption that what was transferred was one form or another of one major internal object or another connected with a super ego or with an internal object that developed prior to the formation of the super ego, and that this internal object would be critical, judgmental, harsh and sadistic. This internal object would also be projected into and onto the analyst, and would be analysed in terms of the relationship that the patient was attempting to form with the analyst. A non-judgmental interpretation of these projections, one which involved both acceptance and understanding, would be curative, because such an interpretation would create affect-laden insight, as a result of which the structure of the personality would change, or more precisely the ego of the patient would change his own internal world. The projections that were the subject matter of the interpretations would involve a repetition of some feature of the internal world that was anchored to historical experience on the 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 7 basis of which the feature was originally formed. As Holmes (1984) has put it ‘…the ‘mutative interpretation’ (brings) together transference, symptoms and childhood experience in one formulation that sees a common pattern running through each’ (2004, p.214). Occasionally psychoanalysts tried to make such interpretations all in one go, but eventually they realised that such interpretations should not occur in one session. In fact, it might take a year or more to put together a so-called ‘complete interpretation’. The next stage in our understanding of transference in terms of Freudian psychoanalysis involved what the young Jung called the ‘transference neurosis’ (Jung, 1946). In a properly conducted analysis patients create the core formation of the problems that brought them into analysis in the first place. Thus, the full neurosis in all its glory is likely to appear within the transference. However, Jung argued that this depended on whether or not the analysand was capable of making a relationship with the analyst, and at the same time of gaining insight into or about this relationship. With respect to ‘introverted’ people, the analysis of the transference neurosis could lead to their becoming more extroverted. At any rate, this was the intention of an analysis. However, in this connection Jung was struggling to make another point, which marks an important development in psychoanalytical thinking, one for which he is not usually given credit. Jung was suggesting that an inability to form a relationship meant that the core of the neurosis could not be captured or made manifest in the treatment relationship. Jung did not quite have the idea of a narcissistic transference, but somehow he asked the right questions about it: could people who were arrested in their development actually form a relationship? Could they form a relationship with an analyst, especially in the sense of forming a transference relationship with him? Was a person who could not form a transference relationship suitable for psychoanalysis? These are big questions. Of course, Jung went on to develop his own form of psychoanalysis in which the interpretation of the transference became a minor concern. 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 8 In contra-distinction to the work of Jung in which he distinguished patients who could form a transference relationship from those who could not, Margaret Little (1951, 1981) introduced the concept ‘transference psychosis’. She suggested that a psychotic transference was based on the repetition of experience that was typical of the first few months of life, during which psychotic anxieties prevailed. Such anxieties were the basis for the later development of psychoses and a variety of features of borderline and narcissistic personality organisation which could be repeated in the transference relationship. Following World War II many psychoanalysts of all persuasions began to focus on preOedipal phases of development and on how they might be manifest in the transference and in the treatment relationship more generally. They hoped that on the basis of this departure it would be possible to work psychoanalytically with more disturbed, ‘difficult’ patients. These psychoanalysts argued that we could not really understand the deeper levels of the unconscious transference relationship unless we also understood the earliest phases of life, which were characterised by projective and introjective identification, in both their normal and abnormal forms. Although the concepts of projective and introjective identification and the central theory of them originated in the writings and teachings of Melanie Klein, starting in the 1930’s but made increasingly clear in the 1940’s and 1950’s, credit for this development in our thinking must also be given to a number of her younger colleagues. 1 The emphasis placed on the importance of ‘working with and in the transference’ is, of course, not confined to Kleinian psychoanalysis specifically or to British psychoanalysis more generally. For example, during the late 1960’s in the United States more and more psychoanalysts began to recognise the curative power of an appropriately timed and empathetic interpretation of the transference. However, they stressed the difficulties presented by the clinical dilemma that if an analyst avoided the emotional turmoil of the transference, little of lasting value would be achieved, but if he did not shy away from it, he would inevitably be 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 9 affected by the work, and forced to confront his own confusions and emotional vulnerabilities hour after hour, and day after day (Bird, 1972). It would always be necessary for a committed psychoanalyst to struggle with this dilemma. On the basis of these developments psychoanalysts came to believe that psychoanalysis was the only form of treatment for virtually all forms of psychological disturbance. TRANSFERENCE PROCESSES: MODIFICATIONS AND PROBLEMS I would now like to draw attention to several problematic aspects of the fashionable focus on transference in clinical work, and indicate the main parameters of what has become common ground in thinking about these processes. The senior members of the Klein school in London (who have done so much to help us understand the importance of transference processes) discuss the analysis of the transference in ways that suggest that there is nothing else to analyse, and that they do nothing else but analyse the transference (Joseph, 1989). However, it seems to me that when contemporary Kleinians say that they are analysing the transference, albeit in terms of the ‘total situation’, they really mean that they are clarifying the treatment relationship in depth and in detail, but not attempting to reconstruct the past on the basis of their knowledge of the present in order to ascertain how the past is presented in the treatment relationship, that is, how it forms the transference, which, traditionally, is the subject matter for interpretation. In other words, contemporary Kleinians do not actually work in the transference as it was originally defined by more classical Kleinians (Spillius, 2004; Hinshelwood, 1999). Pearl King (2004) has referred to this Kleinian development as ‘sick’, and as constituting a perverse development of psychoanalytical theory and technique. Actually, most psychoanalysts continue to believe that interpreting the transference in the more traditional sense of the term to the exclusion of working with all other processes leads to serious distortions to 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 10 clinical communication as well as to the transference itself. For example, in personal correspondence with me, David Scharff, an object relations theorist, wrote: ‘I have been working with this question of the exclusive focus on the transference in the here and now as a way of overlooking most patients’ actual material, and of understanding the way all material relates to transference and countertransference. Of course, everything relates to everything else, but this is not to say that the transference and countertransference is always the important thing in the relationship. Fairbairn said that the most important factor in analytic treatment is the relationship, because without that nothing else mattered – but he did not imply that the thing to do was to focus exclusively on it (and for that matter probably under-did its focus). I have likened the focus on transference to the use of Global Positioning Systems. While the machinery of the GPS is wonderful and certainly fascinating, focus on a journey on the GPS would avoid the purpose of the trip.’ For several decades, most psychoanalyst have argued that in fact the relationship between patient and analyst is extremely complex, involving many strands (Greenberg and Mitchell, 1983). For example, as Freud (1912) was the first to acknowledge, one strand of the relationship might be denoted in terms of patient and analyst saying to one another: ‘Look, let’s think about this together for a moment, and see what this means to you, to me, and to us’. Later, Fenichel (1941) called this strand of the clinical relationship the ‘rational transference’, and much later, L. Stone (1961) referred to this as the ‘mature transference’. However, both concepts are slightly misleading, because Freud, Fenichel and Sterba were trying to distinguish what is essentially non-transferential elements of the clinical relationship from those elements that are essentially transferential. With a slightly different emphasis, Zetzel (1956) introduced the concept of the therapeutic alliance, and later Greenson (1967) discussed the ‘working alliance’. Whether ‘rational transference’, ‘mature transference’, ‘therapeutic alliance’, ‘working alliance’, etc, the ability and willingness to form this kind of relationship with the analyst 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 11 requires a benign splitting of the ego into a reasonable, judging portion and an experiencing portion, the former recognising that the latter is inappropriate in the present and comes from the past (Sterba,1927 ,1940; Fenichel, 1946). In fact, one of the distinguishing characteristics of a successful analysis is that a therapeutic alliance is established, and that it becomes the basis of the work, because ultimately it is the therapeutic alliance that is internalised, and becomes the internal container of the more mature person. It is very difficult to establish and to maintain a therapeutic alliance. Patients should not be obliged to do so, and only a fairly mature patient is able to do so. Moreover, the ability and willingness to establish a therapeutic alliance will be influenced by the transference, which must be analysed in order that a therapeutic alliance can develop. In other words, the development of the therapeutic alliance involves the repetition of past experience with the analyst in the context of the analysis. This can be understood as the essence of an emotionally corrective experience (Alexander and French, 1946). Closely associated with the therapeutic alliance is the so-called ‘real’ relationship between the patient and the analyst. Greenson (1967) suggested that curative processes are based on the real relationship. This is supported by interviewing patients long after treatment has finished: when they are asked ‘What do you remember? What was good for you?’, they answer, ‘Well, I understood why I responded the way I did, but what has stayed with me is the way my analyst smiled at me, the way he shook hands with me; on these occasions I knew that everything was really authentic, and I had never had an authentic experience’. However, it should be acknowledged that real relationship can also be bad, not very good or at least not good enough. Thus, the real relationship may account for the limitations of an analytical experience as well as for the successes of it. Many members of the group of Independent Psychoanalysts of the British Psychoanalytical Society have attempted to deconstruct the relationship between the patient and 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 12 the analyst, and to find ways of working with the processes of which this relationship is comprised (Rayner, 1991; Kohon, 1986). For example, with respect to the affective relationship between patient and analyst, Pearl King (1978) and Adam Limentani (1977) have discussed what they term the ‘general affective response’, which is a natural element in any relationship, and which can and should be distinguished from projective and introjective identification. Sandler (1993) referred to a process of ‘primary identification’, an automatic mirroring process that underlies analytic empathy. 2 Although in due course I will discuss the work of Foulkes (1964, 1975) in connection with transference and countertransference processes in groups, it is important at least to mention here his early discussions of ‘levels of communications in groups’, which are equally pertinent to attempts to understand processes of communication in dyads: the ‘real’ or ‘personal’, the ‘transference’, the ‘projective’ (I would add the ‘introjective’ complementary process) and the ‘primordial’. It is noteworthy that Foulkes was disassociating his work from the ascendant Kleinian perspective that ‘all was transference’, and that transference was comprised completely of projective and introjective processes. (Of course, despite his main interest in the development of group analysis, Foulkes remained a member of the Freud Group of the British Psychoanalytical Society.) Even when it is agreed that the ‘interpretation’ of the transference should be an important focus in clinical work, but perhaps not necessarily the only focus, and even when it is agreed what is meant by ‘transference’, it must also be asked: what does ‘interpretation’ mean? What should be interpreted in terms of what? How much of the work of interpretation should be done by the analyst? What is the clinical value of attempting to make a so-called ‘complete interpretation’? Is an interpretation an attempt to make a scientific explanation based on attempted reconstruction or is it an artistic act of imagination? Should an interpretation be understood mainly as an effort to translate the language of the patient’s unconscious for the 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 13 benefit of the conscious egos of the analysand and the analyst, or more specifically the language of the analysand for the benefit of the analyst, and vice versa? Should this be done in a way that from time to time allows more and more modern translations to be made? In ‘Varieties of transference interpretations: an object-relations view’ (Stewart, 1987) argues that among the various forms of transference interpretation there is one that is virtually destructive: the ‘inauthentic’ interpretation. The essence of an inauthentic interpretation is that it seems to be issued by a robot. Stewart shared this point of view with Greenson (1967) who made similar complaints about somewhat frightened, rigid young analysts. In fact, we have a lot of feelings towards our patients, and the whole point of having an analysis is to free ourselves from not having feelings to having feelings, and to use them in the service of finding an optimal level of responsiveness to the patient. Stewart also argues that it is not necessary to interpret the transference at every moment of time. In fact, in doing so you end up beating a patient over his head, stopping the full development of the transference neurosis or even the transference psychosis. He says that very often the analyst should just shut up! Believe it or not, he says, a lot of clinical work can and should be done in silence, punctuated with non- interpretative remarks like ‘hmm, hmm’. Give people a little space to think, to feel, to see where they are going, to explore a bit, to be tentative, before making a so-called mutative interpretation. Moreover, in the context of a compassionate silence a therapeutic regression sometimes occurs, and as Balint and others pointed out, not only can this amplify and magnify the transference neurosis or transference psychosis, such a regression can be extremely helpful in itself. In another article, ‘Interpretation and other agents for psychic change’, Stewart (1990) argues that in addition to the analysis of the transference, there are many agents for psychic change, for example, extra-transference interpretations of the content of the communications. He recognises that although reconstructions are not necessarily an accurate historical rendition of a 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 14 patient’s life they do help provide a sense of personal location in time and space. Other techniques are appropriate for overcoming various kinds of analytical impasses (Rosenfeld, 1987), like sitting somebody up and saying ‘Now, what’s going on here? Tell me!’, which involves a subtle way of recognising the maturity of the other person. This may be a new experience, and avoids what can be the re-traumatising of a patient by a rigid application of psychoanalytical theory. (I would add that sometimes it is important to use the transference in order to maximise the power of suggestion in the service of helping a patient reach his own goals, although this is obviously more an instrument of ‘therapy’ than of ‘analysis’.) Perhaps transference processes as such need to be interpreted or explained. Priscilla Kauff (1997), a psychoanalytical group psychotherapist, argues that it would be more productive to think about the transference as the outcome of a propensity to relate to the analyst in the present in terms of the past, and not only in terms of the more or less inevitable recreation of the past in the context of the present. This propensity is related to a patient’s inability to experience new events as new. The inability to have a new experience is undoubtedly a character disorder of pre-Oedipal origins. It may even be connected with such phenomena as intense envy of creativity, addictions to dead objects, etc. Nonetheless, Kauff tries to work interpretively almost exclusively in the Here and Now, and to focus on the patient’s capacity to move beyond those early life experiences that might be responsible of the development of the ‘propensity to transfer’. I would suggest that paradoxically this propensity to relate in the present in terms of the past can be taken up in terms of the transference as a repetition of early experience. For example, it might be understood in terms of problems that characterised a shift from mother to father, or from one breast to the other, or from mother to nanny. It might also be understood in terms of the fear and hatred of integration, experienced as parental sexual intercourse that might bring forth sibling children. In other words, the propensity to transfer can be taken up in the Here and 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 15 Now, and interpreted in terms of past experience, perhaps very early past experience, but past experience nonetheless. The propensity to transfer might also be considered in terms of the overwhelming power of what Freud described as the ‘repetition compulsion’, which is a basic element of the psychoanalytical model of the mind. The propensity to transfer can be seen in this way in the malign forms of projective and introjective identification. W. Stone (1997), a psychoanalytical group psychotherapist and self-psychologist, would agree that the transference is a manifestation of a propensity to relate to the analyst in terms of the past, and that this phenomenon has pre-Oedipal origins, but suggests that this propensity to transfer is not inevitable. It is based on particular kinds of narcissistic injury connected with early empathic failures and the absence of self objects who nurtured the development of selfesteem, leading to wishful and compulsive fantasies about being cured in an omnipotent and omniscient way. Not surprisingly, Stone is happy to work supportively, and is less concerned to work interpretatively within the Here and Now. 3 Yet, I would ask whether, if this propensity to relate in the present in terms of the past is analysed successfully, or if the patient is helped no longer to need the analyst as an empathic self-object, and, hence, the transference is dissolved, will the patient no longer have a transference to the analyst? Does this mean that a patient is ‘cured’ or that he will no longer form a transference relationship, which, clearly, is not the same state of mind that Jung first described in patients who were incapable of forming a transference to the analyst? Or does it mean that the content of the communications can be analysed more easily, which is what Freud thought in the first place, that is, a transference neurosis interfered with the analysis of the content of the communications, and was not the sole subject matter for an analysis, and, therefore, that the analysis of the transference neurosis enabled a freer and more productive analysis of the content of the communications? I also wonder if the development from Strachey’s original idea that the mutative interpretation must focus on the bad object in the 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 16 transference, to the current Kleinian idea that this focus must be an exclusive one, is connected with the shift in the patient population from those who are primarily neurotic to those who are primarily character disordered, often with addictions and perversions rooted in a history of extreme traumatic experience. COUNTERTRANSFERENCE: EARLY WORK It is impossible to delay any longer a discussion of countertransference processes, partly because many of the modifications to the classical and even neo-classical theories of transference processes are based on the development of an appreciation and deeper understanding of countertransference processes. Freud (1915) first used the term in ‘Observations on transferencelove’, perhaps for obvious reasons. He did not go into this in great detail, because for him countertransference processes involved an irrational interference which had to be kept in check, even though an analysis was supposed to eliminate this irrational interference. In some ways, Klein agreed with Freud, and was cautious – if not sceptical – about the analyst’s becoming overly involved with using his own feelings as a source of information about the transference (Spillius, 2004). In 1950, however, Paula Heimann argued that the countertransference should be understood as a source of information about the mind of the patient. It is an essential tool for serious clinical work. Winnicott (1949) also wrote a seminal article on projective and introjective identification and the countertransference, ‘Hate in the countertransference’, as did Little (1951) ‘Countertransference and the patient’s response to it’. These authors each stressed that we have to be keenly aware of our own processes of introjective identification and our own internal worlds, in order to follow our own emotional responses and to disentangle them from those that a patient wishes us to have as a way of telling us about his state of mind and past 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 17 experience. We are not sitting there as inorganic objects into which stuff is being put. We are taking stuff in, identifying with it, working with it, trying to understand what is being said and what is being heard, trying to figure out our own contribution to what is, at least in part, a coconstruction of the developing and changing relationship. Moreover, understanding countertransference is essential for understanding psychotic and borderline and narcissistic transferences, and all very deep aspects of unconscious communications. This message was captured in the title of an article written about three decades later by Brenman-Pick (1985) ‘Working through in the countertransference’. During the late 1950’s, however, Winnicott (1960) argued that so many psychoanalysts had begun to use the concept of the countertransference to mean merely their ‘response’ to a patient, and that so many had begun to use the concept to cover a multitude of sins, that it would be best for us to return to the original meaning of the concept, i.e. the intrusion of essentially irrational and non-professional attitudes into the work. I have often heard Hannah Segal say the same thing. This must be one of the few instances of agreement among Freud, Klein, Segal and Winnicott. Furthermore, in agreement with Sandler et al (1973), Kernberg (1984) wrote that the analyst must continuously separate out projected material from his own countertransference disposition in the ‘restricted sense of the term’. As recently as 2002, Springmann, having traced some lines of development in our thinking about countertransference, observed that a certain inconsistency and unclarity characterises the way ‘countertransference’ was initially defined, and the way its implications for clinical work were drawn in terms of whether the existence of countertransference was primarily a problem to be solved by further supervision and analysis, or an ‘indispensable’ communicational, and, therefore, clinical tool. ‘Countertransference’ was used to refer to a broad spectrum of processes, i.e., all the analyst’s feelings towards the patient, some of which are problematic, some useful, and some both, which mainly accounts for the continued and 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 18 continuing confusion. To make matters worse ‘countertransference’ was used to refer narrowly to the transference of the psychoanalyst to the transference of the patient, and to the psychoanalyst’s more general responses to the patient, whether for good or for ill. However, Springmann suggested that ultimately our confusion might be resolved if we were to distinguish between ‘therapist-induced countertransfence’, ‘patient-induced countertransference’, and ‘combined countertransference’, recognising that the most typical form of countertransference is the ‘combined’. According to Springmann, therapist-induced countertransference is more or less the same as Winnicott’s concept of subjective countertransference, and patient-induced countertransference, with Winnicott’s concept of objective countertransference. I would like to quote Springmann at some length, slightly re-ordering his paragraphs: …Therapist-induced-countertransference (my italics) would comprise those parts of countertransference that constitute direct expression of the therapist’s intra-psychic configuration … in the form of current and longstanding unresolved conflicts …(which)… interfere in the therapeutic interaction… by disrupting the therapist’s capacity to perceive the presented material without distorting it, by interfering with his benevolent neutrality or by paralyzing his empathy… (T)herapist-inducedcountertransference would include, beside blind spots, all the therapist’s idiosyncratic reactions to persons in general, or to particular types of persons in particular… personal likes or dislikes, as they might be triggered off accidentally by external circumstances, such as the patient’s physiognomic features, his gestures, or his political opinions… (or)… whenever they are inadvertently allowed to contaminate the therapeutic interaction. Theoretically, the essential, defining factor of therapist-inducedcountertransference that demarcates it sharply from patient-induced-countertransference, is the consideration that the patient, except for being its object and recipient, plays no 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 19 significant part in its creation. To put it differently, therapist-inducedcountertransference is activated by the therapist for reasons that are therapist specific and not patient specific… ‘… (T)herapist-induced-countertransference constitutes that aspect of countertransference, in the traditional, indiscriminate connotation, that should not be allowed to infiltrate and contaminate the therapeutic interaction. Whenever possible, it should be resolved by the therapist without involving the patient…’ ‘…In this context it seems to be justified to paraphrase Freud as follows: “Therapist-inducedcountertransference should be recognized by the analyst in order to be overcome.” Paraphrasing Heimann, as well, it might be said: “The patient ought not to be burdened by therapist-induced-countertransference.” Patient-induced-countertransference (my italics), on the other hand, would comprise all those non-rational intra-psychic manifestations, feelings, fantasies, desires, etc. that become activated in the therapist as a result of the patient’s specific, (usually, but not exclusively, unconscious) active influence. They include the therapist’s deviation from objectivity that, upon being, generally retrospectively analyzed, will be discovered to have been fitting responses to conscious or unconscious corresponding components in the patient’s intra-psychic configuration. They are consciously or unconsciously evoked by the patient as complementary fulfilment of his internal needs, defensive, as in projective identification, or otherwise…the therapist’s personal attributes, his blind spots, distortions, preferences and personal likes and dislikes, as referred to above, will come under the heading of patient-induced-countertransference whenever …the patient has played more than a passive or accidental role in their activation. In these cases it may be presumed that they constituted aspects of the patient’s personality that had found expression via the therapist’s feelings, fantasies, etc…(pp.252-256). 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 20 Springmann goes on to say that in practice therapist-induced and patient-inducedcountertransference are never met in a pure form. On the contrary these components of countertransference are usually discovered intimately intertwined with each other, which is why Springmann uses the concept of combined countertransference to refer to this co-creation by both patient and analyst, which needs to be monitored by them. In sum, as of the mid-1980’s, it was widely accepted that the countertransference is more than merely our own pathological responses to patients, and an indication that we need further treatment. The countertransference is also an essential source of information about our patients. We must be able to use ourselves as communicational tools, reeds in the wind or even as litmus paper. Projective and introjective identifications are the primary means of unconscious communication. However, it is essential both to differentiate those countertransference processes that are induced primarily by the patient from those primarily induced by the therapist, and to recognise that most of the time these two sets of processes are combined. 4 TRANSFERENCE AND COUNTERTRANSFERENCE: THE RELATIONAL PERSPECTIVE Whereas in the mid-1960’s Kernberg was somewhat tentative about how previous developments in our conceptualisation of countertransference processes were likely to influence the future of clinical work, in 1994 Ogden, reminiscent of Winnicott’s famous dictum, observed: ‘There is no such thing as an analysand apart from the relationship with the analyst, and no such thing as an analyst apart from the relationship with the analysand’. In 1995 Gabbard wrote: ‘The perspective that the countertransference represents a joint creation that involves contributions from both analyst and analysand is now endorsed by classical analysts, 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 21 modern Kleinians, relational theorists and so-called social constructivists. Although differences do exist, most contemporary analysts would agree that at times the patient actualises (to use Sandler’s term EH) and internal scenario within the analytic relationship that results in the analyst’s being drawn into playing a role scripted by the patient’s internal world…one of the analyst’s tasks in collaboration with the patient, then, becomes to work his or her way out of the transference-countertransference enactment and understand interpretively with the patient what is going on. In this regard, the intrapsychic and interpersonal realms are joined, and the positivist perspective of the analyst as blank screen is no longer viable. Another task is ongoing self-inquiry and self-analysis. As Schafer has observed: “we may install the analysis of countertransference alongside the analysis of transference and defensive operations as one of the three emphases that define a therapy as psychoanalytic (1992, p.230)”.’ By 1999, however, Hinshelwood was able to assume so much common ground that he attempted to delineate the diversity that characterises this field of inquiry. Today, throughout the world, more and more psychoanalysts, psychoanalytical group therapists and group analysts take a ‘relational perspective’ towards attempting to understand with the patient the transference and countertransference relationship. Although most of us are indeed ‘relational’, only some of us identify with what is currently known as ‘Relational Psychoanalysis’, or refer to ourselves as ‘Relational Psychoanalysts’. This school of thought holds that the transference and countertransference relationship is always co-constructed, and that there are no grounds for the a-priori assumption of clinically informed asymmetry. Some relational analysts believe that we have little need for the two terms ‘transference’ and ‘countertransference’ other than to identify who is the patient and who is the analyst, that is, who is paid and who takes responsibility for the parameters of the 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 22 treatment contract. In fact, many relational psychoanalysts do not refer to the transference but to the ‘co-transference’. It is noteworthy that in his important article on the clinical power of working with and in the transference, Bird (1972) does not refer to the ‘countertransference’ of the analyst but to his ‘transference’ to his patient. 5 Relational Psychoanalysis has a long history. Whereas Ferenczi (1955) warrants special mention, it is not generally remembered that even the classical Freudian Helene Deutsch (1947) stressed that the transference was highly likely to be co-constructed. This school of thought counts among its ancestors most of the fathers and mothers of the Group of Independent Psychoanalysts of the British Psychoanalytical Society, although it must be acknowledged that most of these psychoanalysts would completely eschew the more extreme versions of relational psychoanalysis. Of course, the ancestors of Relational Psychoanalysis also include European and American socio-cultural psychoanalysts. 6 British group analysts have been involved in the development of the relational perspective in dyadic work, but perhaps not intentionally, which may be why psychoanalysts rarely acknowledge their contribution. For years group analysts have argued that there is a lot more to the project of psychoanalysis than the analysis of the transference, emphasising the importance of working with the countertransference, and recognising the power of real relationships. They have acknowledged that during treatment they themselves change, sometimes as a result of the help that is given to them by their patients, and, therefore, that to some extent the whole project is recursive, ideally a matter of a benign circle. Malcolm Pines (1998) has called attention to the importance of Kohut’s (1982) concept of working in the ‘experience near’, which is not quite the same as working within the ‘Here and Now’. Of course, Kohut’s work is extremely important in the development of the relational perspective, mainly in connection with an understanding of the consequences of empathic 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 23 failures on the part of the analyst, and the consequences of this for the treatment relationship. Pines also appreciates Stern and his colleagues’ (1998) concept of ‘moments of meeting’. Following the work of Thomas Szasz (1961), Lionel Kreeger talks about the negotiation of the perceptions of psychic truth in the transference/countertransference relationship. He would ask, “Who can really know what another person’s psychic truth is in the transference and countertransference?’ and he would answer, ‘This is ‘negotiable’.” In other words, Kreeger turns the ordinary English word ‘negotiable’ into a technical concept. However, negotiation is easier said than done, because this kind of negotiation requires an enormous risk. To take an example from outside treatment relationships, many women are always telling their male partners what they feel and what they think, because women believe that men don’t know themselves. After all, they are merely men. However, this requires a degree of caution, because men may feel whatever women want them to feel, or at least say that they do. However, trying to discover what another person feels when it is possible that the other person does not really know what he feels, and when he may be defended against knowing what he feels, requires a great deal of humility and honesty and risk that you may be wrong. This is also true in treatment. When a patient says ‘No, I didn’t say that, I didn’t mean that’, it is necessary to practice what Foulkes called good ‘mental hygiene’, which means that you must be aware of the possibility that you are wrong. You may even have created a patient’s feelings in the transference. What he is feeling at that moment is not really what he feels. In other words, it is necessary tentatively to negotiate perceptions of psychic truth both in thought and in feeling, as well as in fantasy, both intra-personally and inter-personally. According to Nitsun (2001) this attitude of mind is a central feature of the group analytical perspective towards psychotherapy in the dyad. It stems from the fact that group analysts take seriously horizontal, peer-based processes as well as vertical, authority-based processes, which is related to our ability and willingness to use multi-focal vision concerning the 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 24 transference/countertransference relationship as well as other strands of the relationship between patient and analyst. Actually, I would say that group analysts have been instrumental in moving psychoanalytical thinking from mono-focal vision through bi-focal vision to multi-focal vision of the treatment relationship. Several psychoanalytic group psychotherapists in the United States have contributed to the development of the relational perspective in contemporary psychoanalysis. For example, W. Stone (1997) has observed that Alonso (1996) and Rutan and Stone (2000) have contributed to the continuing debate concerning therapist activity, neutrality and self-disclosure. Stone argues that patients who feel held and understood may be more readily amenable to ‘hearing’ and making use of interpretations, and, therefore, it is necessary for the analyst to be more emotionally responsive and transparent in the treatment relationship, and, at times and to a degree, more self-disclosing. The characteristics of the clinician, as reflected in the setting, attitudes towards others, including prejudice, morals and values, etc, contribute to the relationship between the patient and the analyst. Stone writes that these characteristics may be ‘entirely exclusive of and distinct from the transference and countertransference’ (Meissner, 1996, p.25). In order for interpretation to be understood and used in the service of change, it is essential that ‘the patient experiences an ambience in which he/she feels respected, accepted and at least a little understood (Wolf, 1988, p.100)’. Billow (2003) has developed his interest in Bion’s later work into a general relational orientation concerning the analysis of the fear of knowing and defences against this. In his appropriately entitled article ‘Contributions of object relations theory and selfpsychology to relational psychology and group psychotherapy’, Schermer (2000) notes that relational psychoanalysts draw on the ideas of both classical and contemporary object relations thinkers, as well as those of self-psychologists. In other words, the conflicts among these psychoanalysts and their ideas about the origins of object relations and their manifestation 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 25 within the transference and countertransference relationship are overlooked in favour of their common emphasis on the importance of working with and within the relationship between analyst and patient. This has given rise to an extraordinarily complex and pluralistic orientation, one which is proving to be generative. In an article entitled ‘Relational perspectives regarding countertransference in group and trauma’ (pp. 115-136), Rubenfeld summarises what for him is a kind of credo of the relational psychoanalyst or psychotherapist, whether working with groups or individuals, which serves as a unifying principle: A relational/constructivist view incorporates contemporary trends toward viewing countertransference and co-transference as results of mutual intersubjective influence. It moves toward a view of the socially constructed nature of human reality, toward recognising the therapist’s as well as the members’ irreducible individuality and initiative taking, and toward therapy as about meaning-making rather than scientific discovery of The Truth… (p.115). Clearly, there is a basis for various kinds of intellectual and institutional integration of relational psychoanalysis and other contemporary schools of thought. However, I personally am not yet sure whether this is an entirely good thing. I am always in favour of authentic integration, but I wonder whether the development of relational psychoanalysis is more a response to the excesses and distortions of classical and even neo-classical psychoanalysis, and of various developments within it, than it is a psychoanalytical ‘school’ in its own right. After all, if prolonged experience as a patient in psychoanalysis combined with prolonged experience in seminars and supervision does not enhance the ability and willingness of a psychoanalyst to observe and to think and to feel, what is the point of it all? It is sometimes necessary for an analyst to go back into analysis, in keeping with the original Freudian idea, supported by Klein, 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 26 that countertransference is primarily an indication of a problem in listening and hearing. However, rather than automatically going back into a full analysis for difficulties that underpin certain kinds of countertransference processes, it may be sufficient to have colleagues with whom we can and do discuss our work, trusting them sufficiently to give special attention to countertransference processes. Sometimes such groups should be conducted by a group analyst, because this kind of work should not be merely an intellectual activity. 7 SPECIAL THEMES IN THE STUDY OF TRANSFERENCE AND COUNTERTRANSFERENCE All topics in psychoanalysis can be discussed in terms of transference and countertransference, but some are of special interest, because they indicate that the analyst has been negligent, broken clinical boundaries, and has been unethical, although sometimes these transgressions can be rectified by the analyst (Jehu, D., 1994; Gabbard and Lester, 1995). Neglected in the literature and rarely addressed during supervision, at least not while an analyst is in training, the history of the study of these topics is completely intertwined with the history of the study of transference and countertransference processes. A case in point is the erotic transference and countertransference, which is the title of an important collection of papers edited by David Mann (1999). Psychoanalysis has always recognised the importance of erotic desires and their vicissitudes in both normal and abnormal development, and this has been at the centre of clinical work more or less since psychoanalysis was born. Similarly, the manifestation of erotic phenomena within the transference has been a central preoccupation of the psychoanalytical project since the transference was first discovered. Nonetheless, generally the ‘erotic’ has been subsumed under ‘libidinal’, or even under ‘love’, which makes the topic much more acceptable and more amenable to insight. 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 27 The discovery of the transference was based on learning how the analyst’s libidinal desires towards his patients were a source of bias and distortion in analytical work (Freud, 1915). Freud’s early admonitions were addressed towards his more innovative and active colleagues, such as Ferenczi, as well as to the various psychoanalysts who had been drawn to Spielrein (Carotenuto, 1984), who were thought to be putting their patients and themselves, not to mention psychoanalysis, at risk. In any case, during this first phase of our understanding of countertransference processes, those analysts who returned for more personal analysis and supervision were worried about their own impulses to enact their erotic countertransference impulses and fantasies. Most psychoanalysts felt that they should acknowledge such impulses and fantasies, and try to understand and work them through at greater depth than they had been able to manage previously. It was accepted that such desires were unconsciously directed towards pre-Oedipal and Oedipal objects and figures (Searles, 1959), that is, in so far as most analysts were males, towards their mothers and their parts. 8 Of course, there is a significant difference between the erotically tinged transference, at one extreme, and the fully eroticised transference, at the other. 9 In the next stage of our understanding of countertransference processes, we became more aware of how our own various loving and erotic responses to our patients carried essential information about their transferences to us (Gorkin, 1985; Mann, 1995 and 1997; Tauber, 1979 and Tower, 1956). This is especially apparent in our responses to patients who have been sexually abused: countertransference responses that are cold and excessively detached and affectless might involve the communication that the patient’s mother turned a blind eye towards her being abused by her father, living in denial about the incestuous relationships; alternatively, countertransference responses that involve sexual excitement might involve highly seductive challenges to repeat incestuous experiences, perhaps as a test that the patient can be safe in her analysis. 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 28 More recently we have been able to acknowledge the full implications of thinking about the analytical relationship in terms of the ‘clinical couple’, not only in terms of the Oedipal relationships with each and both parents, but also in terms of more mature pairings of various kinds (Kernberg, 1995). For example, Mann (1999) refers to the ‘erotic bond’, which might be conceptualised in terms of its natural history. We have also begun to acknowledge that we ourselves participate unconsciously in the co-creation of the erotic transference. Although we may be able to resist the enactment of our own desires towards our patients, as long as we remain unconscious of such desires, especially if they are split off and denied, and even encapsulated, we are likely to project our desires into our patients, and, thus, collude in the creation of highly charged transferences to us. Such transferences may become exceedingly difficult to contain and to understand, because the patient realises, perhaps more than we do ourselves, that we have invited these responses to us. The awareness of our own participation in the erotic transference and countertransference process can be a source of considerable shame and humiliation, but equally it may be an important – if not essential – step towards the resolution of unconscious conflicts that have paralysed the patient from making more adult relationships. Another interesting topic in the study of transference and countertransference processes is ‘drowsiness and the countertransference’, the title of an important article by Brown (1977). Although drowsiness might seem to be the opposite of erotic desire, these phenomena are closely related, in that they can be defensive against the anxieties associated with one another. Drowsiness on the part of the analyst may be a defence against painful anxieties in response to material that a patient has brought to a session, and more specifically in response to various kinds of projections into the analyst and his internal world. In other words, an analyst becomes drowsy because he is unable to bear the material. This is an example of countertransference in 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 29 the original sense of the term, and when this occurs it behoves the analyst to seek help with his anxieties in connection with the material and the patient who presents it. Drowsiness in the countertransference can, however, also be a response to a patient’s attempt to communicate his state of mind, past experiences and a variety of affects or the absence of them. For example, a patient who has been traumatised tends to create drowsiness on the part of the analyst, not because the analyst needs to avoid specific material, but because he is responding to a patient’s attempts to communicate his assumptions about his mother who he felt turned a blind eye to sexual abuse, or in other words who seemed to have been asleep when the abuse was perpetrated. Drowsiness can be a response to communications about people who were felt to be passive and detached witnesses, not only to sexual trauma, but also to violence, both idiosyncratic and social. For example, patients who have witnessed primal scenes of various kinds tend to create drowsiness in the countertransference, perhaps because they themselves needed to feel drowsy in order to control their own excitement and anger. Drowsiness can also be co-constructed. The analyst who conveys a sense of omniscience and omnipotence is one who must be put to sleep. One motive for this is the wish to punish him for such inappropriate pretence. Another motive is competition and rivalry with the analyst. Still another motive for the creation of drowsiness on the part of the analyst is envy of his alert and thoughtful state of mind, associated with his sense of detachment, neutrality and freedom from emotional turmoil and chaos. Although the patient has contracted with the analyst that he should demonstrate these qualities, they may be perceived as cold inaccessibility. An attitude of excessive detachment may also be a defence against the envy of the patient, which, in turn, may instigate further detachment as a way of not becoming drowsy and so on. In such cases the analyst gets what the patient thinks he deserves: a visit from the Sandman. Another special theme in the study of transference and countertransference processes is the manifestation of traumatogenic processes and their vicissitudes. Although the very birth of 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 30 psychoanalysis was associated with the demotion of crude theories of trauma, if not their refutation altogether, and with the promotion of sophisticated theories of unconscious fantasies originating in instinctual impulses during infancy and childhood, it has taken several generations for psychoanalysts to rediscover the importance of trauma as a source of psychopathology, and to focus on the repetition of traumatic experience in transference and countertransference processes. It is of particular interest to me that in the same way that so many group analysts have contributed to the development of the relational perspective, they have also played an important role in re-introducing psychoanalysts to the study of trauma, especially in the United Kingdom (Garland and Hopper, 1980). They have argued that the tolerant and compassionate management of one’s own countertransference is essential to trauma work. It would seem that the only sin is the enactment within the Countertransference of the transference of the experiences of the attitudes of cold and detached bystanders of the traumatic experience that brought a patient into therapy in the first place (Klein and Schermer (2000); Garland (2003); Hopper (2005); Schermer (2005); Weinberg and Nuttman-Shwartz (2005). THE SOCIAL UNCONSCIOUS AND TRANSFERENCE AND COUNTERTRANSFERENCE PROCESSES 10 As a psychoanalyst and group analyst who was once a sociologist and who still retains a sociological point of view, I want to draw attention to the importance of the sociality of human nature, and to the fact that the constraints of the social unconscious are manifest in both transference and countertransference processes. Pre-Oedipal, Oedipal and post-Oedipal experience must be understood in the context of social, cultural and political factors across the generations. As I (Hopper, 2003a) have discussed in The Social Unconscious: Selected Papers, 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 31 which includes extensive bibliography, the so-called ‘complete interpretation’ of the transference in the ‘Here and Now’ must include not only the ‘Here and Then’, but also the ‘There and Then’ and the ‘There and Now’. Whereas some psychoanalysts have begun to think in terms of a therapeutic triangle (Malan, 1979), that is, in terms of the ‘Here and Now’, the ‘Here and Then’, and the ‘There and Now’, an appreciation of a sociological perspective leads us to think in terms of a therapeutic square, the fourth corner of which is the ‘There and Then’. In other words, in order to understand our relationships to our fathers and mothers, and our fantasies about these processes, we have to understand the various factors that constrain our fathers and mothers. In clinical work it is essential to learn how these transgenerational processes are repeated in transference processes. A few brief examples may serve to illustrate these points. In order to understand what is happening between my male patient and me, it is necessary to understand what happened between my male patient and his father, and what is happening between my male patient and his boss at work; however, it is also necessary to understand what happened between my male patient’s boss at work and his own boss within the context of the power structure of the organisation in which they work, and the prevailing attitudes towards authority and power within their world of work. If I am working with a person who as a child lived in a small Welsh village in the early 1930’s, we will need to think together about the effects of unemployment rates on the gender identity of men in that village, and, in turn, their attitude towards authority in connection with the patient’s relationship to his father, and how this is repeated in his relationship with me. Similarly, if I am working with a post-World War II German, we will need to think together about the difficulties he is likely to have had in identifying with his parents, and how this is repeated in his relationship to me. And if I am working with a woman who is struggling to free herself from the conflicting constraints of gender role definitions that have more or less been ‘deposited’ and perhaps even forced into her mind by traditional parents, we 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 32 will have to work together to understand the comparative importance of the intertwined influences of culture, on the one hand, and parental personalities, on the other, not to mention a variety of family dynamics and sibling relations, all of which will sooner or later be manifest in the transference to me. After all, social, cultural and political factors are involved in the formation of gender identity within the context of family life, and gender identity is completely intertwined with ethnic and class identity, as well as with sexual identity based on the constraints of the body itself. Although Wolstein (1954) outlined the importance of social facts and forces in the determination of the transference, it was really Foulkes (1964) who insisted that working with the social unconscious and the foundation matrix should be a central feature of all clinical work. The point of view that sociality is manifest in the transference and should be interpreted as such, can be traced to the work of several early German psychoanalysts, such as Bernfeld (1929), Horney (1937), Fromm (1930), Waelder (1936) and others. Many group analysts and psychoanalytical group therapists have contributed to the development of this perspective, most notably where British group analysts have helped to found Institutes of Group Analysis, such as Denmark, Germany, Israel, Italy, Norway and so on (Hopper, 2003a). However, the work of American group psychoanalytical group therapists such as Scheidlinger (1964) in his aptly entitled article ‘Identification, the sense of identity and of belonging in small groups’, W. Stone (2004), and H. Kibel (2005) warrants special mention. Although most psychoanalysts in Britain refer to such work as ‘sociology’, several psychoanalysts in the United States have recognised that the self develops through the internalisation of group and family situations and processes, and that such internal phenomena will be manifest in the transference. For example, David and Jill Scharff (1996, 1998) have formulated a contemporary object relations perspective that recognises the power of external whole objects in structuring the internal world, and the re-creation of the internal world within 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 33 many strands of the relationship between patient and analyst. Perhaps special credit should be given to the work of female analysts and feminist analysts in particular. However, Volkan and his colleagues, who might be described as ‘very contemporary object relations psychoanalysts’, have also theorised transgenerational projections, which they discuss in terms of ‘deposited representations’ (Volkan, Ast and Greer, Jr., 2003). They recognise that an analyst may be the recipient of a transference that belongs to his patient almost ‘in name only’, and that his patient may be carrying the material on behalf of a parent or even a grand-parent, and, thus, on behalf of even more distant ancestors. The fact that this work is addressed to social trauma does not mean that it is not valid more generally. In this sense, sociality and the social unconscious are manifest in the transference in terms of Freud’s often overlooked insight that a person’s super-ego is influenced not so much by his parent as by his parent’s super-ego, and so on. Curiously little has been written about the social unconscious and the countertransference in individual work, except by psychoanalysts who are also interested in the study of groups. For example, Bion (1970) discussed the constraints of the Establishment on psychoanalytical thinking, and Racker (1968) referred to the constraints of an analyst’s professional affiliations and institutions on his ‘indirect countertransference’. Citing the work of Dalal (1998) on the unconscious constraints of social beliefs about race, and the work of others concerning nationality, ethnicity and class and other social, cultural and political phenomena, I (Hopper, 1991, 1995 and 2003a) have contributed to our current appreciation of the constraints of the social unconscious on countertransference processes, and on the relationship between the analyst and the patient, partly in terms of what Puget (1986) calls their ‘overlapping worlds’. THE METAPHORIC BASIS OF THE INTERPRETATION OF THE TRANSFERENCE 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 34 The ‘meaning’ of any communication must be examined in terms of multiple, alternative frames of reference, not only as the basis for interpreting the transference, but also for the exploration of the total relationship between the analyst and the analysand. This is a central tenet of ‘Existential Psychoanalysis’, in which the main European players were Binswanger, Boss, Minkowsky, Gebsattel, Kuhn, Caruso, Buytendijk, Bally, and especially Frankl, and the main American players were Allport, Murray, Murphy, Kelly, Maslow, Rodgers and May, as well as Kurt Goldstein, whose early work on the nervous system had influenced Foulkes when the two were still in Germany in the early 1930’s. (Jacob Moreno, the father of psychodrama and sociodrama, drew on these ideas or at least on early versions of them.) It is interesting that although not without inconsistencies and contradictions, the work of the socio-cultural school of psychoanalysis was influential in the early attempts to formulate the principles of Existential Psychoanalysis. Various members of the Group of Independent Psychoanalysts have also been influenced by these ideas, and, in turn, have contributed to the development of the existentialist perspective, for example, Rycroft (1966) and Laing (1967). In Existential Psychotherapy Irvin Yalom (1980) was able to coordinate existentialist ideas into a coherent psychotherapeutic perspective. The importance of considering the metaphoric basis of all interpretations, including the interpretation of the transference, is stressed by Holmes (1984), who was an analysand of Rycroft. He argues that ‘…The task of the therapist is pattern-recognition. In this his own reactions are vital: he has to enter a transferential mode in which he reads the patient’s unconscious responses to treatment as a metaphor for earlier and outer reactions. The process is very similar to the movement that occurs in reading a poem, in moving by metaphor from its outer surface to the deeper meaning. 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 35 Transference and metaphor mean the same thing (Pedder, 1979). Metaphor comes from Greek and transference from Latin but the sense is identical: meta/trans/across – phor/fereo/to carry: both mean to ‘carry across’. Metaphor carries across or links apparent dissimilarities: fact and phantasy, inner and outer, personal and public. It contains what Paul Ricoeur (1979) calls a ‘split reference’ to truth and fiction, like the Majorcan story-tellers who preface their tales by saying ‘it was and it was not’. Transference may be thought of as a special type of metaphor in which early childhood feelings are carried across the relationship with the therapist. Like the poetic metaphor, the transference relationship is both…’ (p.214). In other words, interpretation should be based on our search for the meaning of what transpires within the treatment relationship from the point of view of various frames of reference inherent in a patient’s own life experience. If follows that interpretation is less a matter of the aetiology of psychic reality in terms of past experience, and more a matter of the creation of narrative truth. We should focus less on trying to understand the re-recreation of previous life experience within the treatment relationship, and more on the exploration of the intra-personal and inter-personal dynamics of various ‘spaces’ within the minds of the people involved in the treatment relationship. We should eschew interpretation in favour of clarification. Is it not the case that as we move from conception to death we are always in the state of becoming? Would it not be more helpful to focus on where a person is trying to go, rather than on where he has been, or at least exclusively on where he has been? Should we not wonder what stops him from moving forward? Would it not be better to try to get across the message: stop blaming your parents, stop blaming your constitution, stop blaming your environment, and stop asking your analyst to collude with your celebration of being stuck under the guise of trying to be free? After all, the exclusive focus on the analysis of the transference can become a collusion with the need 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 36 for revenge, and can hide a perverse need to blame and to punish, and a compulsion to stay a victim. (Actually, in Ancient Greek the meaning of the word ‘aetiology’ is to find the cause of an action in order to assign blame and to arrange punishment.) Therefore, would it not be more therapeutic if we shifted our emphasis from the past to the future, to the ‘If and When’ (Scharff, 1998; Hopper, 2003a), which might be considered as another cell in the space/time paradigm. These two basic points, the importance of focusing on the meaning of a patient’s communication from the point of view of alternative ‘meaning schema’, and the importance of shifting the focus of concern from the past to the future, are illustrated in an interesting way by Yalom (1980) in Existential Psychotherapy. He summarises a clinical report by Jung in which Jung explicitly suggested an alternative meaning schema to his patient: …The patient was young, analyzed, secularized, enlightened Jewess with a severe anxiety neurosis. Jung inquired about her background and learned that her grandfather was a rabbi who had been widely regarded as a zaddick, a saint who possessed some sight. She and her father had always scoffed at this nonsense. Jung felt that he had an insight into the neurosis and told her: 'Now I am going to tell you something you may not be able to accept. Your grandfather was a Zaddick… Your father betrayed the secret and turned his back on God. And you have your neurosis because the fear of God has got into you.’ The interpretation, Jung reports, ‘struck like a bolt of lightning.’ That night Jung had this dream: ‘A reception was taking place in my house and, behold, this girl (the patient) was there. She came up to me and asked, ‘Haven’t you got an umbrella? It is raining so hard?’ I found an umbrella and was on the verge of giving it to her. But what happened instead? I handed it to her on my knees as if she were a goddess.’ 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 37 Jung’s dream told him that the patient was not just a superficial little girl, but that she had the makings of a saint. However her life was directed toward flirtation, sex, and materialism. She had no way to express the most essential feature of her nature – namely, that ‘in reality she was a child of God whose destiny (my italics: EH) was to fulfil His secret will.’ Jung told the patient his dream (as was his wont) and his interpretation of it. In a week, he reports, ‘The neurosis had vanished.’ (It is rare, incidentally, for Jung to report a successful brief therapy case.) (pp.476-477). This material illustrates the clinical importance of being able and willing to explore the meaning of the content of a patient’s communications in terms of alternative and multiple frames of reference. It shows how Jung shifted from the patient’s transgenerational past to her future, and not only to her unknown future but to what he regarded as her destiny to fulfil God’s will. In other words, Jung did not focus on her past destructiveness, but on her future possibilities for reparation and forgiveness. Yet, I do not want you to be seduced by the charm and optimism of Yalom’s example and by the charisma of Jung. I want you to appreciate the sheer complexity of these issues, and to wonder why Jung did not try to analyse the girl’s transference to him. For example, I would have wanted to explore the ways in which Jung’s patient had displaced her thoughts and feelings about her father onto her grandfather, the meaning of ‘grand’, the connection between the girl’s fantasies about her father and grandfather and her fantasies about God, and certainly her splitting her body, sexuality and aggression, on the one hand, from her more cerebral and spiritual processes, on the other. I would have been aware that from time to time many of us dream about our patients. Sometimes these dreams are dreamt on behalf of our patients, not merely on behalf of ourselves about our patients (which is itself a group analytical point, that is, dreams can be co-constructed). However, when we have a 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 38 dream about our patients, we are obliged to analyse our countertransference processes in depth and in detail, which may provide important insights into countertransference difficulties as well as into communicational processes that are centred on our countertransference responses. It is not necessarily helpful to tell a patient about the dream that you have had about him or her, but it is always helpful to use your own understanding of the dream in order to understand better the transference and countertranference relationships. I would have thought carefully about my feelings towards this ‘young, analysed, secularised, and enlightened Jewess’. I hope that I would have been aware that I was very taken with her. I am sure that I would have wondered whether my feelings were connected with unresolved Oedipal processes on the basis of which my attraction to my patient might be understood in the context of my feelings about her father and her grandfather, whose identities and traditions were very interesting to me. 11 I would also have wanted to help the patient understand better both her father and her grandfather. Another reservation concerning this Existentialist antidote to the exclusive focus on the transference in terms of a particular psychoanalytical meaning schema, is that many patients are unable to feel that life is ‘meaningful’. This may be based on an inability and unwillingness to make connections both within the mind and between the patient and the analyst and other people, which may be a matter of the patient’s refusal to let ‘things’ come together. This can be understood in terms of fears about parental intercourse and mother’s pregnancy. Blocking perception of such connections is tantamount to blocking the development of a sense of meaning. Winnicott and others have discussed these processes in terms of ‘pee-ing into the intercourse’. Actually, many patients feel compelled to strip and de-nude the meaning schema provided by others of any iota of lively meaning. They are envious of the connections that they perceive in the lives and minds of others. In other words, meaninglessness itself can be taken up in the context of transference and countertransference processes. In fact, it is more helpful to do 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 39 this than to try to provide meaning schema for patients, because many patients are unable and/or unwilling to use the schema provided by the analyst and by others. These various points seem so obvious to me that for many years I have wondered why Yalom used this particular anecdote about Jung’s interpretation in order to illustrate his argument concerning the importance of alternative meaning schema. 12 Although I can see the value in the therapeutic – if not the analytic – attempts to facilitate the development and maintenance of alternative meaning schema, especially for those patients who seem so unable to find one for themselves, I can also see the value of focusing on the analysis of transference and countertransference processes within the context of the total relationship between patient and analyst in order to facilitate a patient’s discovery of a meaning schema that is meaningful to him. PART II TRANSFERENCE AND COUNTERTRANSFERENCE PROCESSES OF INDIVIDUALS IN PSYCHOANALYTICAL GROUP PSYCHOTHERAPY, GROUP ANALYSIS, AND GROUP TRANSFERENCE PROCESSES The history of working with transference and countertransference processes in groups is complex and characterised by intense debate. For example, Slavson, one of the founders of group psychotherapy in the United States and the father of the American Group Psychotherapy Association, was highly doubtful whether a transference neurosis could form and develop in group psychotherapy, much less be analysed within a group (Slavson, 1971). Wolf and Schwartz (1962) believed that whether the profound regression that characterised the transference neurosis would appear in group settings depended on the attitude of the therapist towards this phenomenon, and, therefore, the kind of interventions he made. In many schools of group work the analysis of transference and countertransference processes plays only a minor role, and, 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 40 indeed, there are some in which it plays no role at all. For example, in his famous textbook The Theory and Practice of Group Psychotherapy, which has now gone into its 5th edition, and has sold more than one million copies, Yalom does not include the analysis of transference processes in his list of the ten most curative factors in group psychotherapy. Berne (1960) and many other group dynamicists refused to think about transference processes in general and transference neuroses in particular, because these notions were based on what they regarded as an outmoded psychoanalytical point of view. Whitaker and Lieberman (1964) omitted these terms entirely. In the context of group analysis, Foulkes changed his mind at least twice about the emphasis that he thought should be given to the interpretation of the transference and the transference neurosis in clinical work in groups. In 1957 in Group Psychotherapy: The Psychoanalytic Approach Foulkes and Anthony argued that the group situation is not favourable to the formation of the transference neurosis, but that if and when it does occur, the group setting does not favour its analysis and working through. However, in 1964 in Therapeutic Group Analysis Foulkes wrote that on the basis of twenty years of experience he had changed his mind in that he had observed that individual transference neuroses could be recognised in the group situation, and could, therefore, be analysed and worked though. Yet, in 1975 in Group Analytic Psychotherapy: Method and Principles, he objected to what he called the ‘modern (Kleinian: EH) tendency to place transferential interpretations at the centre of the analytical process’, which he believed could be done but should not be done, because this strengthened the neurosis. Foulkes and Anthony made two basic points about transference and countertransference processes in groups. The first point, to which I referred in my discussion of transference in the dyad in psychoanalysis, is that transference processes are one of the four ‘levels of communication’ in groups; the other three levels of communication were said to be the ‘real’ or ‘personal’, the ‘projective’ and the ‘introjective’, and the ‘primordial’. Foulkes and his 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 41 colleagues assumed that people transferred their past experiences with parents and other ‘whole objects’ in general from early life and perhaps as late as adolescence to the here and now of the group. In this formulation it was assumed that the so-called projective and introjective level of communication referred to internal psychic processes and part objects who or which were not based on actual experience with real people as much as on body-mind interactions which gave rise to fantasies that were formed more or less in parallel with experiences of real parental objects. This internal life was communicated in terms of projections and introjections within the here and now, but not, according to Foulkes, in terms of transference processes as such. The primordial level of communication involved the expression of archetypes and other features of what classical Jungians called the ‘collective unconscious’, based on the structure of the organism and the species. The communication of primordial material was not regarded by Foulkes as a transference process. Personally, I do not think in terms of the collective unconscious in the classical Jungian sense of the concept, and I do not focus on what Foulkes called the primordial level of communication. 13 I doubt whether Foulkes was correct to suggest that part-objects were not a component of the transference level of communication. Moreover, the projective/introjective level of communication may be separate from the so-called ‘personal’ or ‘real’ level of communication, but hardly from the transference level of communication. The second basic point that Foulkes and his colleagues made about transference processes was that from the point of view of each patient in the group, Transference to the Conductor differs from transferences to other patients in the group, to the group as-a-whole, various sub-groups and relationships within the group, various aspects of the context of the group, etc. Similarly, Countertransference from the conductor differs from countertransferences from any one or more members of the group. (The justification for the use of the upper case and the lower case is to indicate who is the official analyst.) It is debatable whether we should refer 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 42 to the transferences from one member of a group to another member of the group as ‘countertransferences’, because in this sense a countertransference is responsive rather than primary, although this is always a matter for negotiation. Of course, most of the time the Transference is primary, not just in the attention of the group analyst, but also in the attention of others in the group. In fact, Foulkes (1964) described the Transference and the transferences in clinical group analysis as being manifest in what he called a ‘continuously re-integrating network’, which he later called the ‘dynamic matrix’ of the group, which is slightly misleading. Foulkes and his colleagues and their followers believed that the complete interpretation of transference and the countertransference processes is much easier to conceptualise in group analysis than it is in psychoanalysis, in which long periods of time are required in order to get the whole picture of the origins of psychic reality, because usually this is expressed in a serial way with respect to the single person of the analyst, like a series of still photographs, rather than like a film using multi-focal perspectives on people, sub-groups, and even the group as a whole. In other words, in groups the multi-personal nature of psychic life is likely to be expressed simultaneously and, so to say, in the round. More specifically, group analysts believe that in groups the Oedipus complex is likely to be more fully presented in transference and countertransference processes than in the dyad. 14 Patterns of Oedipal whole objects and part objects are repeated, that is, all aspects of the mental representation of the bodies and minds of the parents and siblings are presented. In fact, part object configurations are especially apparent in groups. For example, responses to a new member of a group are not only unconscious expressions of feelings about younger siblings, but may also be directed towards the conductor’s penis or breast or a phallic element of the conductor’s mind, etc. either entirely as part objects or in conjunction with whole objects as well. Group analysts understand that there is no such thing as a ‘sibling’, but only a ‘sibling in the context of a family and parental configuration’. 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 43 Group analysts are particularly sensitive to the dynamics of the sociality of each person’s internal world, and believe that the contents of each person’s social unconscious are recreated and made manifest in simultaneous Transferences and tranferences, and Countertransferences. These processes reflect how psychic reality originates and develops, that is, within social situations. Through their regressions, the members of groups tend to recreate their past patterns of functioning in their families of origin as well as their families of pro-creation, at various phases of their development, in addition to past patterns of functioning in groups of all kinds, perhaps starting with play groups and classrooms. Although ways of participating in groups can be traced to the effects of previous experience in groups, and ultimately to early family life, actual experience in groups becomes a source of subsequent experience in groups, and so on. The unconscious constraints of past and present foundation matrices are also manifest in Transference, transference and Countertransference processes. This means that the unconscious constraints of the ever forming and developing dynamic matrix of the group are also manifest in these processes. Pat de Maré (1974) made an important contribution to the group analytical understanding of transference and countertransference processes by individuals in groups when he argued that what he terms ‘transposition’ processes should be distinguished from transference processes. He introduced the concept of ‘transposition’ in order to describe the way a person sometimes perceives that an analyst in the treatment setting is like his father in the domestic setting, or that a group in a clinical setting is like his family. In this case a patient is not imagining the analyst to be his father, or unconsciously forcing him to be his father, but perceiving the analyst to be like his father in the domestic setting that has been transposed onto the clinical setting. In a sense, it is the setting or context that has been transferred from the past to the present or from another place to the present clinical place. For example, the group becomes one’s family of origin or even of pro-creation, or becomes a school classroom, 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 44 sometimes in a fairly concrete way. De Maré stressed that certain feelings and dynamics follow from this transposition of the context of the relationship. He argued that transpositional processes are subject to interpretation, and should be treated in this way. In other words, a patient who says ‘this situation is my family’, at one extreme, or ‘like my family’, at the opposite extreme, is likely to perceive the analyst as ‘being his father’, at one extreme, or ‘like his father’, at the opposite extreme, and that these perceptions should be analysed accordingly. Helen Durkin and Henrietta Glatzer, two psychoanalytical group therapists in the United States, developed their ideas in parallel with Foulkes and Anthony, Bion and Ezriel, although they were informed by their various ideas. I will consider the work of Bion and of Ezriel in due course, but in the first instance it should be recognised that in ‘Transference neurosis in group psychotherapy: the concept and the reality’, published in 1973, Durkin and Glatzer state that very early on they noticed that although the liveliness of group interaction precluded the development of parallel vertical transference structures, and compelled the therapist to focus on the rapidly shifting relationships within the group, all the major aspects of the members’ transference repertoires eventually came into play, and could be analysed, not withstanding the fact that in groups the form and the course of development of transference neuroses stressed the horizontal plane. They adopted Kubie’s (1968) concept of transference processes in preference to what they regarded as the old-fashioned static and rigid concept ‘the transference’. They also accepted Foulkes’ concept of transference processes in clinical groups as a ‘continuously reintegrating network’, and his use of the figure-ground perspective of gestalt psychology as a way of thinking about individuals and groups. (Actually, Foulkes did not really use this phrase ‘continuously re-integrating network’ in order to describe transference processes in groups as much as he used it to describe what he later termed ‘the dynamic matrix’ of the group, which was influenced by the four levels and kinds of communicational processes in groups, the socalled ‘transference level’ being one of them.) However, Durkin and Glatzer argued that since it 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 45 is the individual who comes for help, it must be his individual transferences that are resolved, and ‘…that it is possible to achieve this goal in the group… (T)he transference distortions lock members into unrealistic relationships and create communication jams (resistance). As these are systematically analysed, group psychotherapy becomes a genuine and intensive emotional experience (Durkin, 1964). The resulting behaviour modifications can be measured in terms of concrete changes in the communications and the behaviour, which may be linked, point for point, with the resolution of transference resistances. Structural change is the end result of working through all the ramifications of each member’s transference distortions. It is in this sense that we speak of resolving individual transference neuroses in group therapy.’ (p.186). Durkin and Glatzer concluded ‘…there is no level of fantasy or conflict that cannot be re-experienced and resolved by systematic analysis of the intra-group transferences. (p.188). ‘At each step of the analysis of transference neuroses in the group all the members participate in their own ways (defences) and share in the experience and its analysis. The individual must be analysed, but not to the neglect of the other members who are interacting with him…’ (pp 197198). …(T)he course of the transference neurosis is less continuous than in individual analysis and is more likely than in dyadic work to be interrupted and changed in its focus. Moreover, a brand new transference might easily be evoked by a group reaction or event. … (T)his discontinuous quality does not obstruct the development of the transference neurosis but facilitates the working through process, because the same 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 46 material will come up again and again with different members in various kinds of group situations until it has been worked through.’ (p.198). Many questions can and should be asked about transference processes and transference neuroses in groups. Some clinicians argue that these processes are less intense in group analysis than they are in dyadic treatments, and, therefore, that group analysis is the treatment of choice for people who tend to get overly enmeshed in sticky, clingy and perhaps parasitic transferences in dyads (Stein, 1963; Pines, 1998; Hopper, 2003b). However, other clinicians believe that transference processes are more intense in groups than in dyads, partly because of the depth and spontaneity of regression in groups (Ethan, 1978), and, therefore, that people who cannot handle the intensity of group regression will do better in a dyadic form of treatment. Still other clinicians argue that both points of view are correct, but that the intensity of these processes and the ability to work effectively with them depend on the type of patients (Kibel, 1992; Horwitz, 1994). It is, of course, important to consider the topic of Countertransference processes in groups. Although many group analysts and psychoanalytical group therapists draw on the work of object relations thinkers who have studied the importance of countertransference processes, ranging from Bion to Turquet to Kernberg to Hinshelwood, to name only a few who have also written about group dynamics, others have been influenced by the work of Kohut and his followers with respect to the consequences of the failure of the therapist to maintain an empathic orientation. Foulkes was the first group analyst who recognised that the conductor of the group may be both a subject and an object of emotionally corrective transmuting internalisation. The relational perspective has become increasingly important in group analysis and psychoanalytical group therapy (Billow, 2003), partly because the notion of the ‘co-transference’ has particular 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 47 validity in the context of group work generally, not only between members of a group but also between the conductor and any one or more members of the group. A vital and unique feature of psychoanalytical group psychotherapy and group analysis is that the group can and often does help the analyst with his Countertransference, especially when it has been induced by a patient in the group (Hopper, 2005). We all have blind spots, and we can all be disturbed, especially when we are working with difficult patients, who are so good at confusing us. It is well known that the problems of narcissistic therapists can be exacerbated in groups, because the narcissistic therapist and the group may regress in ways that amplify the collusion between them, leading to fixed patterns of idealisation, the projection of all negativity, justified or not, into the context of the group, and in extreme cases to the emotional abuse of more vulnerable patients (Horwitz, 2000). However, there is nothing like the maturity of a well functioning group to help the analyst with his blind spots. Sometimes the group offers interpretations, and can take over the analyst’s role, which gives him time and space to think in situ. This cannot happen within the clinical dyad. Although on rare occasions the participants in the dyad may consult a third party, usually such input is in the form of consultation to or supervision of the analyst. Actually, Ormont (1970-71; 1991), following Winnicott, refers to pathological countertransference as ‘subjective’ countertransference, and to induced countertransference as ‘objective’ countertransference, and encourages us to use the group in our attempts to resolve subjective countertransference, in the same way that we use objective countertransference to resolve group resistances. The importance of receiving what is in effect ‘supervision’ from the group, or perhaps being able to work with the group as though the members of it were always potentially cotherapists, is especially relevant when working with groups of traumatised people or groups in which there has been a surfeit of trauma (Schermer, 2005). A group who feels that their various 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 48 forms of suffering have been accepted by the therapist, will, in turn, be more than willing to accept his vulnerabilities and frailties. In sum, most group analysts and psychoanalytical group therapists firmly believe that despite a number of variations on the theme, not only can transference processes, transference neuroses and even transference psychoses be analysed in groups, it is essential to do so. However, I personally doubt whether in comparison to what is possible in the dyad such processes can be analysed in depth and detail, that is, to the point of resolution. I suppose that it is relevant to remind ourselves that this is not really an either/or question, because we can and do work in dyadic and group treatments combined, both serially and simultaneously. In some countries combined therapy is standard practice. GROUP TRANSFERENCE PROCESSES I have been considering transference and countertransference processes by individuals in groups. I will now considerer the so-called ‘group transference’, that is, a collective transference of the whole group, or a transference that is shared by members of the whole group, to a particular object who they hold in common, such as their group conductor or to the evolving dynamic matrix of the group. 15 In fact, the classical psychoanalytical definition of a group is a collection of people who have projected their ego ideals into the same person, who then becomes the leader of the group. It follows from this perspective that the very essence of a group as opposed to a collection of individuals is that a collective transference has occurred. It also follows that a thorough analysis of this collective transference is likely to lead to a dissolution of the group, that is, to a shift from a so-called group to a so-called collection of individuals. This would not be a matter of either a regression or a progression, but a shift from what might be regarded as 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 49 one ‘position’ to another, perhaps like a shift from ‘aggregation’ to ‘massification’, or from ‘fight’ to ‘flight’. I will return to these positional shifts in due course. Many psychoanalytical group therapists argue that a so-called ‘group transference’ is meaningless (Ferreira, 1980). They argue that even if the members of a group do hold certain objects in common, they have no pre-group experience in common that is available for the Transference and the transferences to the objects in the group who they hold in common. This idea has found widespread support among many psychoanalytical group therapists, perhaps those in the United States in particular (Durkin and Glatzer, 1973), who tend to hold ideologies of individualism, and seem not understand the concepts of the dynamic matrix and the foundation matrix. They hold dichotomised conceptions of the individual and the group, and seem not to understand that the individual and the group are two sides of the same coin. More specifically, they lack a concept of the person, that is, an individual suffused with sociality (Hopper, 1982), and do not respect the existence of ‘social reality’, concepts of which are regarded as fantasies. In contrast, I believe that so-called ‘group transferences’ do occur, and that attempting to understand and to work with such phenomena gives group analysis its unique clinical power. Thus, I also believe that groups exist qua groups, as do other kinds of social system, and possess characteristics and dynamics of their own. These characteristics and dynamics are partly independent of the personalities of their members, on the one hand, and of features of their wider social contexts, on the other. Persons create groups and are created by them, which has always been true and which will always be true, and, therefore, persons in groups form various kinds of transferences within groups, and groups form various kinds of transferences to their common objects. I will now indicate several different kinds of group transference within the context of progressive psychoanalytical models of group dynamics and development. 16 Some 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 50 psychoanalytical group therapists and group analysts who accept the reality of a group transference assume that the members of groups have had certain experiences in common by virtue of the fact that they are human beings, or more precisely human organisms or members of the species homo-sapiens. Thus, the members of groups have had similar, if not identical, experiences as infants in relationships to their parents, both in mind and body. These experiences can be described in terms of psychoanalytical models of psycho-sexual development, i.e. the oral, anal, phallic, genital and perhaps adolescent phases involving particular instinctual impulses, defences, fantasies, object relations, etc. These assumptions have given rise to a variety of theories and descriptions of phases of group regression and group development that are independent of the personalities of the members of the group, and independent of the constraints of particular societies and cultures within which the group exists. For example, group development is thought to be based on the appearance and resolution of the Oedipus complex during the group’s phallic phase, when all the members of the group are likely to regard the conductor or leader of the group as an ambivalently loved father whose authority has to be challenged and modified, at least by the males in the group. (Most theorists of this ilk have neglected to discuss contributions to group transferences from the female members of the group, and to my knowledge have never studied group transferences of an all female group.) Groups become more cohesive if and when their members are able to mobilise a challenge to the leader of the group, and discover that the leader can ‘take it’ or that they can replace him, and then move on. Such models of group regression and group development have been discussed in depth by Saravay (1978), who also provides extensive bibliography on this topic. An especially refined version of this psychoanalytical theory of stages of group regression and group development according to psycho-sexual stages of individual development, was proposed by Slater (1966), who drew extensively from Totem and Taboo (Freud, 1913) and from Experiences in Groups (Bion, 1962), as well as from empirical data. Slater was interested 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 51 primarily in the evolution of religious structures and beliefs. In response to an ‘abstinent’ leader, the members of a group are seen to create a shared group fantasy of an omniscient and omnipotent protector who will make order from the chaos of their experience. When this deification fails, the group moves to a stage of revolution during which themes of deicide, scapegoating and cannibalism emerge. The third stage is characterised by identifications with and incorporations of the leader in a way that allows the group to believe that they, too, can become ‘parents’, and do the things that parents do. Slater suggests that women encourage this revolt and welcome the sexuality of the males, but, in a sense, remain comparatively passive. The fourth and final stage is characterised by what Slater calls ‘the new order’, something like a utopia or even what Bion regarded as an ideal type of ‘work group’. These stages are thought to be more or less inevitable, and, therefore, during each stage the group regard the official leader, as well as one another, in stage-specific terms, which are, in effect, ‘group transferences’. Slater calls these group transferences ‘microcosms’. Such microcosms are sometimes thought to be based on the primordial archetypes of the collective unconscious both in the personal and the group sense of this concept. Another psychoanalytical approach suggests that the members of a group tend to experience the group and the conductor of it as very ‘large’, powerful and resourceful. Thus, they tend to experience the group as a mother or parts of her, in terms of both positive and negative transferences, at every level of psycho-sexual development (Scheidlinger, 1968), and the conductor or leader of the group as father or as parts of him, and the members of the group as the mother’s other children. However, such Transferences and transferences may be reversed, that is, the group may be perceived as father, and the conductor as mother. Various patterns of splitting and projection and displacement occur. Although the members of a group vary in how they experience particular objects, there is no doubt that they tend to experience the group and its members in terms of an ‘archaic family pattern’ (Schindler, 1951). 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 52 Basic assumptions can be considered as properties of a group that have been co-created in terms of a collective transference from mother’s mind and body to the group-as-a-whole, often focusing more on part objects than on whole objects (Bion, 1961). Some theorists have hypothesised that basic assumptions are not merely analogous to, but actually homologous with, specific stages of group regression and group development, i.e. (ba) Dependency with the oral stage; (ba) Fight/Flight with the anal stage; and (ba) Pairing with the phallic stage. Other kinds of theorists, especially those who work with a version of a Kleinian model of development, refer to (ba) Dependency as an expression of envy and idealisation associated with the paranoid/schizoid position; (ba) Fight/Flight, as an expression of envy and denigration associated with the paranoid/schizoid position; and (ba) Pairing as an expression of sexuality as a manic defence against the anxieties associated with the depressive position. Of course, although Kleinians themselves do not regard these ‘positions’ as phases of development, they acknowledge that in the first instance they appear in sequence. I personally regard the basic assumptions as ‘interpersonal forms of defence’ against the experience of psychotic anxieties, i.e. (ba) D is an interpersonal defence against paranoid schizoid anxieties, envy and idealisation; (ba) F/F, against paranoid schizoid anxieties, envy and denigration; and (ba) P is an interpersonal defence against depressive anxieties (Hopper, 2003a). However, whether in terms of phases of development or of non-sequential forms of interpersonal defence against psychotic anxieties, or both, basic assumptions arise among regressed people in groups, and only in groups, and not within isolated individuals or even within dyads. Groups can manifest simultaneously group transferences and countertransferences, individual Transferences and Countertransferences, and individual transferences and countertransferences within groups. Through an awareness of all three sets of phenomena it is possible to facilitate the integration of intrapersonal and interpersonal life. This idea derives from Bion’s theory of the valence that a particular person might have for a role associated with a 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 53 particular basic assumption, although Kernberg (19xx) prefers Redl’s (19xx) concept of role suction to the concept of valence, and I prefer Foulkes’ and Moreno’s concept of personification. I would like at least to indicate here that I (Hopper, 2003b) have tried to develop a theory of a fourth basic assumption (or a first, depending on whether (ba) D is regarded as first or a third) called Incohesion: Aggregation/Massification or (ba) I: A/M, which I regard as an interpersonal defence against the psychotic anxieties associated with the fear of annihilation following traumatic experience (Hopper, 2003b). In this basic assumption the group oscillates between a state of aggregation, that is, a state in which the group is a collection of more or less isolated individuals, like a collection of billiard balls, and a state of massification, that is, a state in which the group becomes a merged mass, like several warm wet sponges squeezed together. In this theory, traumatic experience is hypothesised to be primary and envy secondary, which is in essence an interpersonal theory of the human condition from the moment of conception. In other words, it is hypothesised that envy is likely to arise as a defence against feelings of helplessness, and that helplessness is more likely than envy to be the essence of the human condition. With respect to the aggregation pole of Incohesion, I discuss the role of the ‘lone wolf’, a highly withdrawn isolate. Drug addicts are often lone wolves, and I present a case of a drug addict who in the middle of a group took a joint from behind his ear and lit it up and started to pass it around. A group offers a role for a withdrawn isolate like this. Even if the lone wolf expresses all sorts of aggression and repeats all sorts of things that went on in his family, he can do it safely in the group. He can take a toque in order to withdraw from the heat of the group, and although quite frankly I would prefer that he didn’t, I can tolerate it and the group can tolerate it. And with respect to the massification pole of Incohesion, I discuss the role of the ‘cheerleader’ or the ‘morale booster’, who covers up feelings of depression and an inability to function by repeating over and over again that this is the greatest group that he has ever been in. 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 54 Such a person often comes from a family in which there was a great deal of morale boosting and cheerleading in order to avoid thinking about all the problems that threatened the integrity and the cohesion of the family. When groups are characterised by the basic assumption of Incohesion: Aggregation/Massification as a particular form of group transference, they also offer very anxious people particular skins of identity, and, therefore, they provide important opportunities for clinical work with individual transference neuroses and psychoses. Ezriel’s (1950) work on ‘central group tensions’ should also be understood in terms of both group and individual transference and countertransference phenomena combined, addressed to the group-as-a-whole in terms of the mind and body of the mother, and, I think, the father as well. Ezriel argued that central group tensions tend to be co-created in terms of ‘required relationships’ in order to defend against the feelings and fantasies associated with ‘avoided relationships’, because, in turn, the avoided relationships might lead to ‘catastrophic relationships’. Ezriel’s work consisted of elucidating these patterns of group transference, and then engaging in an exploration of the contribution made to them by each individual member of the group. Ezriel thought that working with these individual processes was essential to clinical work in groups. There is another kind of group transference that requires our special attention. It is very different from the other processes that have been regarded as group transferences, i.e. the group as an organism and/or as a person (from the point of view of, say, Slater), the group as mother (from the point of view of Scheidlinger, Schindler and others), basic assumptions and valences as forms of interpersonal defence against shared anxieties connected with deep regressions in response to the group as the mind and body of the mother (from the point of view of Bion and other group relations thinkers), and central group tensions as forms of interpersonal defence against similar anxieties, also based on regression (from the point of view of Ezriel). I have in mind that sometimes the members of a group unconsciously co-create within the 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 55 dynamic matrix of their group various situations that exist within their wider social, cultural and political contexts, that is, within their foundation matrix. The concept of foundation matrix really implies transgenerational processes, and, therefore, the features of the foundation matrix that are co-created may have occurred ‘far away and long ago’. (I tend to use Slater’s term ‘microcosm’ in order to denote these intra-group phenomena, although Slater used the term only to refer to the unconscious co-creation of early developmental patterns from a Freudian point of view.) These situations in the foundation matrix are co-created within the group in the form of a collective transference to the objects who the group hold in common, such as the conductor, the dynamic matrix of the group, various sub-groups, etc. Group microcosms are not merely a matter of so-called ‘parallel processes’, because there are causal connections between co-creation of the intra-group microcosm and the experience of members of the group of the particular contextual situations that they have cocreated. These microcosms can be regarded as ‘equivalent’ to particular situations in their foundation matrix, and these processes of co-creation can be regarded as processes of ‘equivalence’. Equivalence is based on projective and introjective identifications in the service of attack, expulsion, control and above all on non-verbal communication, primarily in an effort to produce a narrative of unspeakable pain and suffering. Thus, these causal connections are based on feelings of helplessness and loss, and of the inability to mourn both authentically and completely, and can be considered in terms of ‘chosen trauma’ and ‘chosen glories’ that are often transmitted across the generations (Volkan, Ast and Greer Jr., 2003). Group microcosms, however, do not always reflect traumatogenic processes. They may also reflect the foundation matrix of the group in more general ways, including systems of interaction, normation, communication, styles of thinking and feeling, styles of leadership, followership and bystandership, etc. Although I reject most aspects of metaphorical Darwinian models of the history of social, cultural and political arrangements, it is sometimes useful to 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 56 regard intra-group microcosms based on equivalence with situations in the group’s foundation matrix, as ‘memes’ (Dawkins, 1982). Memes are said to be elementary particles of culture which are analogous to genes, and which people propagate to a greater or lesser degree because they are appealing and/or useful, especially to those who are in positions of power and influence. The tendency to produce these forms of group transference depends on the degree of homogeneity within the group concerning the particular situations that are unconsciously felt to be either oppressive, on the one hand, or desirable and useful, on the other. However, even groups who are highly heterogeneous with respect to a particular situation may co-create a microcosm of that situation in so far as it is felt to be important to a particular member of the group or to a particular sub-group. Although groups tend to focus on the mental life of the conductor, each and every member of the group may become the focus of these co-created microcosms. It is always difficult to know how such information is picked up, but I have no doubt that it is. Most likely this should be regarded in terms of the projective and introjective level of group communication. It is important to stress that in all microcosms based on equivalence as a form of group Transference to the conductor, and of group transferences to participants in the group and to other group-based objects, including the dynamic matrix of the group itself and various subgroups, etc., all the members of the groups participate in their own way. Personal processes overlap with group processes. Naturally, not every one is sucked into group processes to the same degree; some are leaders, some are followers, some are collusive bystanders, and some are rescuers. I would also stress that the delineation of such processes requires very careful and painstaking exploration and negotiation before the hypothesis is offered that the group has in fact unconsciously co-created a microcosm of a situation from its context about which the members of the group have strong, complex and largely unconscious feelings and fantasies that they are crying out to express and to have understood. 17 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 57 Social dreaming (Lawrence, 2000) is yet another kind of group Transference. This phenomenon has long been recognised and appreciated by group analysts (Kreeger, 1975), who have observed that in contrast to the more classical psychoanalytical theories of dreams and dreaming, people can and often do dream for one another, not only in dyads but also in groups and even in large and more complex social systems. Social dreaming does not have to be taken up by a conductor or convenor of the social system in question in terms of a group transference, but these interpersonal and collective dreams do involve group transferences to the conductor and to other objects who the group holds in common. It would be inappropriate to present here a more detailed description and discussion of social dreaming. In sum, group analysts very much appreciate the reality of the group-as-a-whole, and not merely in terms of metaphoric concepts of it. They also try to make clinical use of their understanding of social reality. In other words, they appreciate the possibilities of applying an understanding of group dynamics to clinical work. For group analysts this is not merely an academic exercise in social psychology. However, for most of us the constraints of working only in terms of the models developed by psychoanalytical group therapists, family pattern therapists, Bion and his followers, Ezriel, etc, have proved to be too limiting. This is not to say that their insights should not be part of the repertoire of a group analyst; in fact, it is hard to imagine how we might work without the benefits of their contributions. However, it is equally hard to imagine how we might work without the benefits of the Foulkesian project, that is, understanding the power of a group and its members to produce a dynamic matrix of which they are largely unconscious, in the context of a foundation matrix of which they are also largely unconscious. I say ‘largely unconscious’, because I am sure that we would all agree that it is impossible for any of us ever to be completely conscious of internal and external constraints. CONCLUDING REMARKS 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 58 As I indicated at the very start of this monograph, ‘transference’ and ‘countertransference’ are meaningless concepts unless they are used to refer to processes located within the context of treatment relationships, because in a very real sense transference and countertransference processes involve the essence of the human condition, implying that we are all born and live within the constraints of particular historical ‘junctures’, and have a propensity to present our pasts and to experience our presents in terms of our pasts. However, it seems to me that it might be useful to extend our study of transference processes by specifying a variety of contexts within which these processes occur and might be considered in a systematic way. For example, relations between teachers and students within the classroom group warrant further study (Slavin, 2002), as do all situations in which authority structures are paramount, ranging from a bus conductor and a passenger in the context of the bus, to a sales assistant and a customer within the context of a shop, but much more importantly to a General Practitioner and a patient within the context of a clinic, to a financial adviser and a client within the context of a bank, etc. However, this is a topic for another study. I also began by insisting that any discussion of transference processes must be contextualised in terms of a more general philosophical and psychoanalytical point of view. I will conclude in the same way, because in asking you to reconsider the meaning of transference and countertransference processes and the importance of working with them, I am really asking you to think about the meaning of hope (Hopper, 2003a, 2003b). Clearly, this is a very complex topic, and I can only suggest and imply the main elements of my argument. I am not interested in what might be regarded as ‘infantile’ hope or ‘pie in the sky’ hope, but in ‘mature’ hope, which has its own natural history in every individual within his own social, cultural and political context. I define mature hope as the ability and willingness to exercise the transcendent imagination. I am interested in how a person imagines that he can make his life better: not just how it might have been, but how it might be, and what he plans to do about this. The ‘If and 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 59 When’, based on hope defined as an expression of the transcendent imagination, may be expressed in terms of an attempt to imagine an optimistic ‘scenario’, to embrace the idea of moving forward, of refusing to get bogged down and to dwell in the past. This kind of developmental achievement is, of course, based on having been able to mourn our losses sufficiently to have created the space that the capacity to imagine new and more optimistic scenarios requires. The desire for revenge must give way to the desire for repair and forgiveness. And when an appreciation of reality suggests that obstacles and frustration are inevitable, it is important to be able to identify with the achievements of others. It is imperative to make and to maintain empathic connections with people whose interests are in conflict with our own, and with people who will still be alive after we die: children and grandchildren, but also, at least for me, students and even patients, not to mention friends and colleagues, and in a more distant and abstract way fellow citizens in general. Thus, mature hope depends on social ligaments that connect us not only to the past, but also to the present and to the future. Difficulties in the development and maintenance of hope in this sense of the term can and should be taken up within the context of transference and countertransference processes, both in dyads and in groups. Clearly, the struggles to protect and nourish the good object must be encouraged, or at least interpreted, in the context of the recognition of the power of the bad object, and the need to make use of the energy of the bad object or at least the need to keep it contained. A few psychoanalysts from various schools of thought have acknowledged the importance of attempts to understand the formation, development and maintenance of what they variously term ‘new’objects (Baker, 1993) and ‘transformational’ objects (Bollas, 1979). Spillius (2002) emphasises the importance of our thinking together about ourselves, others and relationships in a ‘new way’. Loewald (1980) was one of the first psychoanalysts to underscore the importance of conveying such attitudes to patients who struggle to balance the analysis of their ‘past presented’ with the need to formulate alternative ways of living. American self- 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 60 psychologists stress the importance of being forward looking and of being able to make changes, e.g. Ornstein (1992), Tolpin (1998), and Stone (2003). The early work of Balint (1965) concerning regression and the possibility of ‘new beginnings’ should not be overlooked. Nor should Zinkin’s (1998) work on the possibilities for the emergence of new realities and perceptions of them. We may have to change our circumstances before we can change our minds, which is what Foulkes meant when he said that sometimes insight follows change rather than the other way around. In essence, this is a Marxist point of view in that the super-structural and the personal are based on the sub-structural and the collective. Actually, we know that economic and social development gives rise to a finely graded system of stratification, containing many middle classes, a free and equal access to an education system, and maximum economic and social mobility, all of which, in turn, give rise to a general sense of mature hope, and disorders of entitlement or disorders of hoping must always be understood within this broader context. Thus, the psychoanalytical and the psychotherapeutic project must have a political dimension. This perspective underpinned the early ideas of Foulkes concerning ego-training in action as one of the therapeutic activities offered by group analysis, an idea that was developed by Brown (2000) in his work on ‘self development through subjective interaction’. Political movements and religious movements are often closely related, sometimes as partners and sometimes as antagonists. It is very difficult to discuss hope without considering what people believe about the finite dimensions of life of this earth. For example, we know that a society in which the vast majority of people are frozen into abject economic, social and political poverty, and a small elite are born into power, favours a belief in a good life after death, which becomes a substitute for mature hope during this life. Of course, Born Again Christians emphasise the importance of a belief in ‘Christ-in-life’, and not only ‘Christ-in-death’, which favours a way of life in which people are encouraged to actualise their desirous expectations, 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 61 and to regard spirituality as more than merely the acceptance of pain and frustration. However, it is entirely understandable that the psychoanalytical and the psychotherapeutic project should also have a religious dimension. In fact, psychotherapists have been called ‘secular priests’ (North, 1972). 18 I am tempted to go so far as to suggest that working within the transference might even enhance a patient’s ability to be ‘spiritual’. Let me explain. Some people can perceive material facts, but not psychic or social facts, such as their own minds or those of others, or they can perceive bodies but neither persons, groups, interpersonal processes or group processes. Such people are quick to embrace the idea that there is no such thing as a ‘society’. However, an appreciation of the non-material is closely related to an appreciation of the spiritual. Might it be possible to understand the inability and/or refusal to perceive the ‘non-material’ and the spiritual in terms of an inability during infancy to perceive the mind of the mother and/or of the father? More importantly, might this insensitivity to the non-material and to the spiritual be based on the conviction that one’s own mind and ‘heart’ have never been perceived and appreciated by others, particularly parents? If so, this is bound to be repeated in transference and countertransference processes. Thus, through analysis of these processes we can increase the ability to be both psychologically and sociologically minded as well as spiritually minded. In other words, working with psychic and social reality and psychic determinism within the transference and countertransference relationship does not preclude an interest in the nature of what transpires between people. The increased ability and willingness to perceive the ‘new’, which is always a confirmation that a change has occurred, means that further change might be possible. APPENDIX I 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 62 A brief note on the theory and concept of the social unconscious with respect to individuals and groups I have discussed the theory and concept of the social unconscious at some length in my (Hopper, 2003a) The Social Unconscious: Selected Papers. I will only summarise a few basic points here. The ‘social unconscious’ refers both to the fact that people can be and often are unconscious of social factors and forces, and to the social factors and forces of which they are unconscious, in exactly the same way that the notion of ‘unconscious’ generally refers both to the fact that people can be unconscious of a variety of biological and psychological factors and forces, and to those biological and psychological factors and forces of which they are unconscious. Actually, there really should be no need for the concept of social unconscious other than to denote the social (and the cultural, economic, political, etc. but as in the social sciences the term ‘social’ is used to include these phenomena in general) nature of a particular object of which people are unconscious. Of course, human nature is always biological, psychological and social, and such factors and forces are completely intertwined. The personal is always interpersonal (and familial, group, organisational, and societal) from conception to death. In other words, the ‘social unconscious’ refers to the constraints of social objects that have been internalised, that is, to aspects of the ‘social world’ or to the foundation matrix including those aspects of it which involve deposited representations that have been projected across the generations. Social objects are internalised in the same way that all external objects are internalised: on the basis of negative processes involving identifications with aggressors of various kinds, and of positive processes involving identifications with loving and nurturing objects of various kinds. However, the emphasis here is on understanding that external objects can be internalised in more or less their pristine forms, that is, uncontaminated by prior projections. Recognising 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 63 this possibility is virtually a psychoanalytical heresy. A third way through which external social objects in particular are internalised is through instinctually and physiologically governed mirroring processes, which may be related to the constraints of mirror neurones. However, the processes of internalisation of social objects require some sort of processes of engagement by the other. For example, it is highly unlikely that processes of internalisation by the infant of the mother are driven merely by the actions of mirror neurones, and are most certainly likely to be governed by the actions of the mother as well – if not primarily. Many Jungians use the ‘collective unconscious’ as a synonym for the ‘social unconscious’. However, there are important differences between these two concepts. The ‘collective unconscious’ emphasises what Jungians call ‘archetypes’ and archetypical phenomena, unconscious fantasies of complex social situations and figures within them which are said to be inherited on the basis of acquired characteristics that are rooted in situations that occurred eons ago. This Jungian point of view is virtually identical to the old, classical point of view that Freud (1913) expounded in his speculative but influential Totem and Taboo. However, traditionally Jungians have gone so far as to locate these primary situations in myth and fable, for example, regarding figures such as Zeus and Athena as our ‘original’ father and mother, not only in narrative but also in fact. Of course, other, more contemporary Jungians use the ‘collective unconscious’ in order to stress the importance of socialisation processes, in which case the concept is almost the same as the ‘social unconscious’. I personally do not think about the dynamics of groups and other social systems in terms of their so-called ‘social unconscious’ or their so-called ‘collective unconscious’. I do not believe that social systems have minds, conscious or otherwise. In order to have a so-called ‘mind’, it is necessary to have a brain. Social systems do not have brains. Similarly, I eschew phrases such as ‘collective memory’ and even ‘public opinion’, except in terms of statistical data. Of course, the metaphor that social systems are like people, but not that they have brains or 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 64 even minds in the same way that people do, is an extremely useful heuristic device that directs our attention and curiosity towards certain parts and aspects of social systems of which people are unconscious. This is especially apposite under conditions of trauma in which both wounded people and the systems of which they are members regress in ways that involve a sense of interpersonal merger as a defence against the fear of annihilation and group fragmentation. Unfortunately many people tend to think more concretely about an unconscious mind of the group, organisation, family or even of the society as a whole, and they use the concepts of the social unconscious and of the collective unconscious in order to refer to the existence of the putative unconscious mind of a social system, in which case the analogy between a group and an organism or person becomes an homology, and what has begun as an useful heuristic device, becomes a very limited device implying stability rather than change, the value of the existing power structure, and that somehow the people in power are always seen as the brain and heart of the group, and those without power as the group’s stomach and genitals. (Of course, machines and mechanistic analogies and homologies have the opposite implications, and they too are very limiting.) Also, given that the ‘collective unconscious’ usually refers to primordial archetypes and archetypical phenomena with respect to individual persons, its applications to groups is especially confusing, pace Foulkes’ reference to the primordial level of communication. In order to refer to those aspects of social systems of which their members are unconscious, I would prefer to use concepts such as the ‘shared unconscious’ or ‘interpersonal unconscious’. The first of these is popular in some circles of Jungian analytical psychologists, and the latter, in some circles of psychoanalysts who have been influenced by the work of Fairbairn and other British object relations theorists, as well as some Foulkesian group analysts, who cite the fact that in his brief discussion of the concept of the social unconscious Foulkes himself referred to ‘interpersonal’ processes. 19 However, I am not really happy with either of these terms, mainly because they are based on analogies and homologies which are almost 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 65 always more trouble than they are worth, confusing the personal with the systemic levels of analysis, and misusing the insights afforded by the theory of living open systems. When working with what might be regarded metaphorically as the unconscious of a societal social system, I do not necessarily refer to phenomena such as myths, fables, great literature, music, structural dilemma and contradictions, etc. Such phenomena are not necessarily elements of the so-called ‘unconscious’ of the society, because the members of the society are not necessarily unconscious of such material. However, this is an old story of sorts, in that often people become more conscious of those processes of which they have been less conscious, and as and when they do, then, by definition, they are no longer unconscious of these processes. Of course, groups and other component social systems of a society will manifest the foundation matrix of the society. Although individual and group analysis offers the possibility for becoming more conscious of the constraints of the foundation matrix, usually the conductor of a group shares the same society and culture with the other participants in it, and he is not necessarily more conscious of the foundation matrix and its constraints than are the participants themselves. However, when I have conducted groups in other societies and cultures, I have been able to help the participants in them to elucidate these elusive constraints, precisely because I was much less constrained by them than they were. References Alexander, F. and French, T.M. (1946). Psychoanalytic Therapy Principles and Application. Lincoln and London: University of Nebraska Press. Alonso, A. (1996). Toward a new understanding of neutrality. In L.E. Lifson (ed.) Understanding Therapeutic Action: Psychodynamic Concepts of Cure (pp. 3-19). Hillsdale: NJ: Analytic. Bacal, H.A. (eds) (1998). Optimal Responsiveness: How Therapists Heal Their Patients. 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 66 Northvale, NJ.: Jason Aronson. Baker, R. (1993). ‘The patient’s discovery of the psychoanalyst as a new object.’ International Journal of Psycho-Analysis, 74, 1223-1233. Balint, M. (1965). Primary Love and Psycho-Analytic Technique. New York: Liveright. Benjamin, J. (1995). Like Subjects, Love Objects: Essays on Recognition and Sexual Difference. New Haven, CT: Yale University Press. Bennis, W.G., and Shepard, H.A. (1956). ‘A theory of group development.’ Human Relations, 9, 415-438. Berman and Weinberg, H. (2004). International Journal of Group Psychotherapy. Berne, E. (1960). ‘Psychoanalytic versus dynamic group therapy.’ International Journal of Group Psychotherapy, 10, 98. Bernfeld, S. (1929). ‘Der soziale Ort und seine Bedeutung für Neurose, Verwahrlosung und Pädagogik.’ Imago XV, 2, 17-24. Billow, R. M. (2003). Relational Group Psychotherapy: From Basic Assumptions to Passion. London: Jessica Kingsley Publishers. Bion, W.R. (1962). Learning from Experience. London: Heinemann. Bion, W.R. (1970). Attention and Interpretation. London:Tavistock. Biran, H. (2005). Discussion of ‘Progress in object relations theory and group analysis: from classicism to the influence of social forces’. Plenary Lecture given by Dr Howard Kibel at the Congress ‘The Power of the Group Space’ sponsored by the Israeli Association for Group Psychotherapy. Tel Aviv, Israel, July. Bird, B. (1972). ‘Notes on transference: universal phenomenon and hardest part of analysis.’ Journal of the American Psychoanalytic Association, 20, 267-301. Blum, H.B. (1973). ‘The concept of the erotized transference.’ Journal of the American Association, 21, 61-76. 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 67 Bollas, C. (1979). ‘The transformational object.’ International Journal of Psycho-Analysis, 60, 97-197. Bollas, C. (1987). The Shadow of the Object. London: Free Associations Books. Bowlby, J. (1982). Attachment and Loss. (2nd Edition). New York: Basic Books Brenman-Pick, I. (1985). ‘Working through in the countertransference.’ International Journal of Psychoanalysis, 66, 157-166. Brown, D. (1977). ‘Drowsiness in the countertransference.’ International. Review of Psychoanalysis, 4, 481-492. Brown, D. and Zinkin, L. (2000). The Psyche and the Social World: Developments in Groupanalytic Theory. London: Jessica Kingsley Publishers. Carotenuto, A. (1984). A Secret Symmetry: Sabina Spielrein Between Jung and Freud. London: Regan & Kegan Paul. Casement, P. (2002). Learning from our Mistakes. London: Brunner-Routledge. Dalal, F. (1998). Taking the Group Seriously. London: Jessica Kingsley Publishers. Dawkins, R. (1982). The Extended Phenotype: The Gene as the Unit of Selection. London: Freeman. de Maré, P. (1972). Perspectives in Group Psychotherapy. London: Allen and Unwin Ltd. de Maré, P. and Kreeger, L.(1974). Introduction to Group Treatment in Psychiatry. London: Butterworths. Deutsch, H. (1947). The Psychology of Women. London: Research Books Ltd. Durkin, H.E. (1964). The Group in Depth. New York: International Universities Press. Durkin, H.E. (1971). ‘Transference revisited.’ International Journal of Group Psychotherapy, 21, 11. Durkin, H.E. and Glatzer, H.E. (1997). ‘Transference neurosis in group psychotherapy: the 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 68 concept and the reality.’ International Journal of Group Psychotherapy, 47, 183-199. (Original work published 1973). Durkin, J.E. (1981). Foundations of autonomous living structures. In J. Durkin (ed.) Living Groups (pp.24-59). New York: Brunner/Mazel. Epstein, L. and Feiner, A. (eds) 1979. Countertransference. New York: Jason Aronson. Ethan, S. (1978). ‘The question of the dilution of transference in group psychotherapy.’ Psychoanalytic Review, 65, 569-578. Ezriel, H. (1950). ‘A psychoanalytic approach to the treatment of patients in groups.’ Journal of Mental Science, 96, 774-79. Fairbairn, W.R. (1952). Psychoanalytic Studies of the Personality. London: Routledge & Kegan Paul. Fenichel, O. (1941). ‘The ego and the affects.’ Psychoanalytic Review, XXVIII. Fenichel, O. (1946). The Psychoanalytic Theory of Neurosis. London: Routledge and Kegan Paul. Ferenczi, S. (1955). Final Contributions to the Problems and Methods of Psycho-Analysis. New York: Brunner/Mazel. Ferreira, A.G. (1980). ‘Transference and transference neurosis in group analysis.’ GAIPAC, XIII/2, 93-99. Field, N. (1992). ‘The way of imperfection.’ British Journal of Psychotherapy, 9, 2-11. Foulkes, S.H. (1937). ‘On Introjection.’ International Journal of Psychoanalysis Foulkes, S.H. (1964). Therapeutic Group Analysis. London: Allen & Unwin. Reprinted in 1984, London: Karnac. Foulkes, S.H. (1975). Group Analytic Psychotherapy: Methods and Principles. London: Interface, Gordon & Breach. Reprinted in 1986, London: Karnac. Foulkes, S.H. and Anthony, E.J. (1957). Group Psychotherapy: The Psychoanalytic Approach. 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 69 London: Karnac, 1984. Foulkes, S.H. and Prince, G. (eds) (1969). Psychiatry in a Changing Society. London:Tavistock. Fowles, J. (1969). The French Lieutenant’s Woman. London: Vintage Classic (Reprinted 2005). Freud, S. (1912). The Dynamics of Transference. Standard Edition, Vol. XII. London: The Hogarth Press. Freud, S. (1913). Totem and Taboo. Standard Edition, Vol. XIII. London: The Hogarth Press. Freud, S. (1914). Remembering, Repeating and Working Through. Standard Edition, Vol. XII. London: The Hogarth Press. Freud, S. (1915). Observations on Transference-Love. Standard Edition, Vol. XII, 157-174. London: The Hogarth Press. Fromm, E. (1930). The Working Class in Weimer Germany: A Psychological and Sociological Study, trans. Barbara Weinberger, Cambridge, Mass: Harward University Press. Reprinted in 1984. Fromm, E. (1956). The Art of Loving. New York: Harper and Row. Fromm-Reichmann, F. (1950). Principles of Intensive Psychotherapy. Chicago: Chicago Universities Press. Gabbard, G. and Lester, E.P. (1995). Boundaries and Boundary Violations in Psychoanalysis. New York: Basic Books. Gabbard, G.O. (1995). ‘Countertransference: the emerging common ground.’ International Journal of Psychoanalysis, 76, 3, 475-485. Glatzer, H.T. (1962). ‘Narcissistic problems in group psychotherapy.’ International Journal of Group Psychotherapy, 12, 448. Glatzer, H.T. (1969). ‘Working through in analytic group psychotherapy.’ International Journal of Group Psychotherapy, 19, 292. Gorkin, M. (1985). ‘Varieties of sexualised countertransference.’ Psychoanalytic Review, 72, 3, 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 70 421-440. Greenacre, P. (1954). ‘The role of transference.’ Journal of the American Psychoanalytical Association, 2, 671-684. Greenberg, S. and Mitchell, S. (1983). Objects Relations in Psychoanalytic Theory. London: Harvard University Press. Greenson, R.R. (1967). The Technique and Practice of Psychoanalysis. London: The Hogarth Press. Hamilton, V. (1996). The Analyst’s Pre-Conscious. Hillside, N.J.: The Analytic Press. Heimann, P. (1950). ‘On countertransference’. International Journal of Psychoanalysis, 33, 8184. Hinshelwood, R.D. (1994). Attacks on the reflective space: containing primitive emotional states. In V.L. Schermer & M. Pines (eds). Ring of Fire (pp.86-106). London: Routledge. Hinshelwood. R.D. (1999). ‘Countertransference.’ International Journal of Psychoanalysis, 80, 797-818. Hoffman, I. (1983). ‘The patient as interpreter of the analyst’s experience. Contemporary Psychoanalysis, 19, 389-422. Holmes, J. (1984). ‘The language of psychotherapy: metaphor, ambiguity, wholeness’. British Journal of Psychotherapy, 1, 4. Re-published in 20th Anniversary Issue 1984-2004, 21,2, 209-229. Home, J. (1966). ‘The concept of the mind’. International Journal of Psychoanalysis, 47, 1, 4249. Hopper, E. (1982). A Comment on Professor M. Jahoda’s ‘Individual and Group’. In M. Pines and L. Rafaelsen (eds) The Individual and The Group. New York: Plenum Press. Hopper, E. (1991). ‘Encapsulation as a defence against the fear of annihilation’. The International Journal of Psychoanalysis, 72, 4, 607-624. 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 71 Hopper, E. (1995). ‘A psychoanalytical theory of drug addiction: unconscious fantasies of homosexuality, compulsions and masturbation within the context of traumatogenic processes’. The International Journal of Psychoanalysis, 76, 6, 1121-1142. Hopper, E. (2003a). The Social Unconscious: Selected Papers. London: Jessica Kingsley Publishers. Hopper, E. (2003b). Traumatic Experience in the Unconscious Life of Groups. London: Jessica Kingsley Publishers. Hopper, E. (2005). ‘Countertransference in the context of the fourth basic assumption in the unconscious life of groups.’ International Journal of Group Psychotherapy, 55, 1, 87114. Horney, K. (1937). The Neurotic Personality of our Time. New York: W.W. Norton. Horney, K. (1945). Our Inner Conflicts. New York: W.W. Norton. Horwitz, L. (1994). ‘Depth of transference in groups.’ International Journal of Group Psychotherapy, 44, 271-290. Horwitz, L. (2000). ‘Narcissistic leadership in psychotherapy groups.’ International Journal of Group Psychotherapy, 50, 2, 219-236. Jehu, D. (1994). Patients as Victims: Sexual Abuse in Psychotherapy and Counselling. London: John Wiley & Sons. Joseph, B. (1989). ‘Transference: the total situation.’ International Journal of Psychoanalysis, 66, 4, 447-454. Joseph, B. (2003). ‘Ethics and Enactment.’ Psychoanalysis in Europe, 57, 147. Jung, K. (1946). The Psychology of the Transference. In Collected Works, 16. London: Routledge and Kegan Paul. Kauff, P. (1997). ‘Transference and regression in and beyond analytic group psychotherapy: 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 72 revisiting some timeless thoughts.’ International Journal of Group Psychotherapy, 47, 2, 201-210. Kelman, H.C. (1999). ‘The interdependence of Israeli and Palestinian national identities: The role of the other in existential conflicts’. Journal of Social Issues, 55, 3, 581-600. Kernberg, O. (1965). ‘Notes on countertransference’. Journal of the American Psychoanalytic Association, 13, 38-56. Kernberg, O. (1995). Love Relations. New Haven, Ct: Yale University Press. Khan, M. (1963). The Privacy of the Self. London: Hogarth Press. Kibel, H. (1992).The clinical application of object relations theory. In R.H. Klein, H.S. Bernard and D.L. Singer (eds.) Handbook of Contemporary Group Psychotherapy (pp. 141176). Madison, CT: International Universities Press. Kibel, H. (2005). ‘Progress in object relations theory and group analysis: from classicism to the influence of social forces’. Plenary Lecture sponsored by the Israeli Congress ‘The Power of the Group Space’. Tel Aviv, Israel, July. King, P. (1978). ‘Affective response of the analyst to the patient’s communication’, International Journal of Psychoanalysis, 59, 329-334. King, P. (2004). What Has Happened to Psychoanalysis in the British Society? In A. Casement (ed) Who Owns Psychoanalysis. London: Karnac. Klein. M. (1952). The origins of transference. In The Writings of Melanie Klein, Volume III, London: Karnac Books, 1993. Kohon, G. (1986). The British School of Psychoanalysis: The Independent Tradition. London: Free Association Books. Kohut, H. (1982). ‘Introjection, empathy and the semi-circle of mental health.’ International Journal of Psychoanalysis, 63, 395-407. König, K. (1987). Transference in groups: Internal fantasy and external reality. 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 73 Group Analysis, 20, 4, 291-305. König, K. (1995). Countertransference Analysis. Northvale: Jason Aronson Inc. Kubie, L. S. (1968) ‘Unsolved problems in the resolution of the transference.’ Psychoanalytic Quarterly, 37, 331. Laing, R. (1967). The Politics of Experience. London: Penguin. Langs, R.J. (1976) The Bi-Personal Field. Aronson: New York. Laplanche, J. and Pontalis, J.B. (1973). The Language of Psychoanalysis. London: The Hogarth Press. Lawrence, G. (2000). Social Dreaming@ Work. London: Karnac Books. Levenson, E.A. (1994). ‘Beyond countertransference.’ Contemporary Psychoanalysis, 30, 691707. Limentani, A. (1977). ‘Affects and the psychoanalytic situation.’ International Journal of Psychoanalysis, 58, 2, 171-197. Little, M.I. (1951). ‘Countertransference and the patient’s response to it.’ International Journal of Psychoanalysis, 32, 32-40. Little, M.I. (1981). Transference Neurosis and Transference Psychosis: Towards Basic Unity. New York: Jason Aronson. Loewald, H. (1980). Papers on Psychoanalysis. New Haven: Yale University Press. MacKenzie, K.R. (1997). Time Managed Group Psychotherapy: Effective Clinical Applications. Washington, D.C.: American Psychiatric Press. MacKenzie, K.R. and Livesley, W.J. (1983). A developmental model for brief group therapy. In R.R. Dies and K.R. MacKenzie (eds.) Advances in Group Psychotherapy: Integrating Research and Practice. (pp. 101-116). New York: International University Press. Malan, D. (1979). Individual Psychotherapy and the Science of Psychodynamics. London: Butterworths. 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 74 Mann, D. (1995). ‘Transference and countertransference issues with sexually abused patients.’ Psychodynamic Counselling, 1, 4, 542-559. Mann, D. (1997). Psychotherapy: An Erotic Relationship – Transference and Countertransference Passions. London: Routledge. Mann, D. (ed) (1999). Erotic Transference and Countertransference: Clinical Practice in Psychotherapy. London and New York: Routledge. Maroda, K. (2004). The Power of Countertransference. (2nd Edition). London: The Analytic Press. McDougall, J. (1995). The Many Faces of Eros: A Psychoanalytic Exploration of Human Sexuality. London: Free Association Press. Meissner, W.W. (1996). The therapeutic alliance and the real relationship in the analytic process. In L.E. Lifson (ed.) Understanding Therapeutic Action: Psychodynamic Concepts of Cure (pp.21-39). Hillsdale, NJ: Analytic. Meltzer, D. (1974). ‘Narcissistic foundation of the erotic transference.’ Contemporary Psychoanalysis, 10, 311-316. Mennecke, B.E., Hoffer, J.A. and Wynne, B.E. (1992). ‘The implication of group development and history for group support system: theory and practice.’ Small Group Research. 23, 524-572. Michaels, R. et al (eds) (2002) Key Papers on Countertransference. London: Karnac Books. Mitchell, S. (1988). Relational Concepts in Psychoanalysis: An Integration. Cambridge, MA: Harvard University Press. Mitchell, S., and Aron, J. (1999). Relational Psychoanalysis: The Emergence of a Tradition. Hillsdale, NJ.: The Analytic Press. Money-Kyrle, R.E. (1956). ‘Normal countertransference and some of its deviations.’ International Journal of Psychoanalysis, 37, 360-366. Reprinted (1978) The 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 75 Collected Papers of Roger Money-Kyrle. Perth: Clunie. Nitsun, M. (2001). ‘Towards a group-analytic approach to individual psychotherapy.’ Group Analysis, 34, 4, 473-484. North, M. (1972). The Secular Priests. London: George Allen & Unwin Ltd. Ogden, T.H. (1994). Subjects of Analysis. Northvale, NJ.: Jason Aronson. Ormont, L. (1970-71). ‘The use of the objective countertransference to resolve group resistances.’ Group Process, Winter: 96-111. Ormont, L. (1991). ‘Use of the group in resolving subjective countertransference.’ International Journal of Group Psychotherapy, 41, 433-447. Ornstein, A. (1992). ‘The curative fantasy and psychic recovery: Contribution to the theory of psychoanalytic psychotherapy.’ Journal of the American Psychoanalytical Association, 39, 377-397. Pedder, J. (1979). ‘Transitional space in psychotherapy and theatre.’ British Journal of Medical Psychology, 52, 37-58. Pines, M. (ed) (1998). Circular Reflections. London: Jessica Kingsley Publishers. Puget, J. (1986). Personal communication concerning what she calls ‘overlapping worlds’. Racker, H. (1968). Transference and Countertransference. London: Hogarth Press. Rayner, E. (1991). The Independent Mind in British Psychoanalysis. London: Free Association Books. Ricoeur, P. (1979). The Metaphorical Process as Cognition, Imagination and Feeling. In S. Sacks (ed.) On Metaphor. London: University of Chicago Press. Rosenfeld, H. (1965). Psychotic States. New York: International Universities Press. Rosenfeld, H. (1987). Impasse and Interpretation. London: Tavistock. Rubenfeld, S. (2005). ‘Relational perspectives regarding countertransference in group and 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 76 trauma.’ International Journal of Group Psychotherapy, 55, 1, 115-136. Rutan, S. and Stone, W. (2000) Psychodynamic Group Psychotherapy (3rd edn). New York: Guilford. Rycroft, C. (1966). Psychoanalysis Observed. London: Constable. Sandler, J. et al (1970). ‘Basic psychoanalytic concepts: eight special forms of transference.’ British Journal of Psychiatry, 1, 17, 561-568. Sandler, J., Dare, C. and Holder, A. (1973). The Patient and the Analyst. The Clinical Framework of Psychoanalysis. London: Allen and Unwin. Revised and expanded by J. Sandler and A.U. Dreher (1992). London: Karnac. Sandler, J. (1976). ‘Countertransference and role responsiveness. International Review of Psychoanalysis, 3, 43-47. Saravay, S.M. (1978). ‘A psychoanalytic theory of group development.’ International Journal of Group Psychotherapy. 28, 481-507. Schafer, R. (1992). Retelling a Life. New York: Basic Books. Scharff, J. (1992). Projective and Introjective Identification and the Use of the Therapist’s Self. Northvale, NJ.: Aronson. Scharff. D. (1996). Object Relations Theory and Practice. Northvale, NJ.: Aronson. Scharff, J. and Scharff, D.E. (1998). Object Relations Individual Therapy. Northvale, NJ.: Aronson. Scheidlinger, S. (1960a). ‘Group process in group psychotherapy: I. current trends in the integration of individual and group psychotherapy’. American Journal of Psychotherapy, 14, 104-120. Scheidlinger, S. (1960b). ‘Group process in group psychotherapy: II current trends in the integration of individual and group psychotherapy’. American Journal of Psychotherapy, 14, 346-363. 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 77 Scheidlinger, S. (1964). ‘Identification, the sense of identity and of belonging in small groups’. International Journal of Group Psychotherapy, 14, 346-363. Scheidlinger, S. (1968). ‘Concept of regression in group psychotherapy.’ International Journal of Group Psychotherapy, 18, 20. Scheidlinger, S. (1974). ‘On the concept of the “mother group”.’ International Journal of Group Pschotherapy, 24, 417-428. Schermer, V. L. and Klein, R.H. (1996). ‘Termination in group psychotherapy from the perspective of contemporary object relations theory and self psychology.’ International Journal of Group Psychotherapy. 46, 99-115. Schermer, V. L. (2000). ‘Contributions of Object Relations Theory and self-psychology to relational psychology and group psychotherapy.’ International Journal of Group Psychotherapy, 50, 2, 199-218. Schindler, W. (1951). ‘Family pattern in group formation and therapy.’ International Journal of Group Psychotherapy, 1, 100-105. Searles, H. (1959). ‘Oedipal Love in the Countertransference’. In Collected Papers on Schizophrenia and Related Subjects (1965). London: The Hogarth Press. Searles, H. (1979). Countertransference and Related Subjects. New York: International Universities Press. Segal, H. (1981). The Work of Hanna Segal. New York: Aronson. Slater, P. (1966). Microcosm: Structural, Psychological and Religious Evolution in Groups. New York: John Wiley and Sons. Slavin, R. (2002). ‘Operative group dynamics in school settings: structuring to enhance educational, social and emotional progress.’ Group, 26, 4. Slavson, S. (1971). ‘Transference neurosis in group psychotherapy.’ Paper presented at the A.G.P.A. Conference. 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 78 Spector-Person, E. (1985). ‘The erotic transference in women and men: differences and consequences.’ Journal of the American Academy of Psychoanalysis, 13, 159-180. Spillius, E. (2002). ‘Understanding oneself and being understood: experiences of supervising psychoanalysts and psychotherapists.’ EPF Bulletin, 56, 5-16. Spillius, E. (2004). ‘Melanie Klein revisited: Her unpublished thoughts on technique.’ The Bulletin of the British Psychoanalytical Society, 40, 4, 13-28. Springmann, R. (2002). Dialogues with Schizophrenia: The Art of Psychotherapy. (4th revised Edition). Broadway, VA: Loafin Tree. Stein, A. (1963). ‘Indications for group psychotherapy and the selection of patients.’ Journal of the Hillside Hospital, 12, 145-155. Sterba, R. (1927). ‘Ueber latente negative uebertragung.’ Internationale Zeitschrift für Psychoanalyse, XIII. Sterba, R. (1940). ‘The dynamics of the dissolution of the transference resistance.’ Psychoanalytic Quarterly, 9, 363-379. Stern, D.N. et al (1998). ‘Non –interpretative mechanisms in psychoanalytic therapy: The “something more” than interpretation’. International Journal of Psychoanalysis. 80, 4, 685-718. Stewart, H. (1987). ‘Varieties of transference interpretations: an object-relations view’. International Journal of Psychoanalysis, 68,197-205. Reprinted (1992) in Psychic Experience and Problems of Technique. London: Routledge. Stewart, H. (1990). ‘Interpretation and other agents for psychic change.’ The International Review of Psycho-Analysis 71, 61-70. Reprinted (1992) in Psychic Experience and Problems of Technique. London: Routledge. Stewart, H. (1992). Psychic Experience and Problems of Technique. London: Routledge. 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 79 Stone, L. (1961). The Psychoanalytic Situation. New York: International Universities Press. Stone, W. (1997). ‘Transference neurosis in group psychotherapy: the concept and reality.’ International Journal of Group Psychotherapy, 47, 2, 211-226. Stone, W. (2003). ‘Strivings and Expectations: An examination of process in groups for persons with chronic mental illness.’ Psychoanalytic Inquiry, 23, 678-696. Stone, W. (2004). ‘Group-as-a-whole: a self-psychological perspective.’ Unpublished paper. Storolow, R. and Atwood, G. (1992). Contexts of Being: The Intersubjective Foundations of Psychological Life. Hillsdale, NJ: The Analytic Press. Storolow, R., Atwood, G., and Brandchaft, B. (eds) (1994). The Intersubjective Perspective. Northvale, NJ.: Aronson. Strachey, J. (1937). ‘On the nature of therapeutic action in psychoanalysis. International Journal of Psychoanalysis, 18, 139-45. Sullivan, H.S. (1964). The Fusion of Psychiatry and the Social Sciences. New York: Norton. Szasz, T. (1961). The Myth of Mental Illness. New York: Hoeber-Harper. Tauber, E.S. (1979). ‘Countertransference Re-Examined’. In L. Epstein and A.H. Feiner (eds). Countertransference. New York: Aronson. Thompson, C. (1964). Interpersonal Psychoanalysis. (ed. M. Green). New York: Basic Books. Tolpin, M. (1998). Matt’s ‘oxygen providing’self-object transference. Presented at the annual meeting of the American Group Psychotherapy Association, Chicago, February. Tower, L. (1956). ‘Countertransference.’ Journal of the American Psychoanalytic Association, 4, 224-255. Truffaut, F. (1973). Day for Night. Tubert-Oklander, J. (2005). ‘I, thou, and us: relationality and the interpretative process in clinical practice.’ Psychoanalytic Dialogues. Tubert-Oklander, J. and Hernandez de Tubert, R. (2003). Operative Groups: The Latin- 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 80 American Approach to Group Analysis. London: Jessica Kingsley Publishers. Tuckman, B.W. (1965). ‘Developmental sequence in small groups.’ Psychological Bulletin, 63, 384-399. Volkan, V., Ast, G. and Greer, Jr.,W.F. (eds) (2003). The Third Reich in the Unconscious: Transgenerational Transmission and its Consequences. New York, London: BrunnerRoutledge. Waelder, R. (1936). ‘The principle of multiple function: observations on over-determination.’ Psychoanalytic Quarterly, 5, 45-62. Weiner, S. (2005). ‘On the difficulty of knowing who is feeling what about whom.’ Whitaker, D. and Lieberman, M. (1964). Psychotherapy Through the Group Process. New York: Winnicott, D.W. (1949). ‘Hate in the countertransference.’ International Journal of Psychoanalysis, 32, 32-40. Reprinted in Through Paediatrics to Psychoanalysis, 194203. NewYork: Basic Books (1958). Winnicott, D.W. (1956). Primary Maternal Preoccupations. In Collected Papers: Through Paediatrics to Psycho-Analysis, pp.300-305. New York: Basic Books. Winnicott, D.W. (1960). ‘Countertransference’. In The Maturational Processes and the Facilitating Environment, pp.158-178. London: The Hogarth Press. Wolf, A. and Schwartz, E.K. (1962). Psychoanalysis in Groups. New York: Grune and Stratton. Wolf, E. (1988). Treating the Self: Elements of Clinical Self Psychology. New York: Guilford. Wolstein, B. (1954). Transference: Its Meaning and Function in Psychoanalytic Therapy. New York: Grune & Stratton. Yalom, I. (1980). Existential Psychotherapy. New York: Basic Books. Yalom, I. (1985). The Theory and Practice of Group Psychotherapy. New York: Basic Books. Zetzel, E.R. (1956). ‘Current concepts of transference.’ International Journal of 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 81 Psychoanalysis, 37, 369-376. Zinkin, H. (ed) (1998). Dialogue in the Analytic Setting: Selected Papers of Louis Zinkin on Jung and on Group Analysis. London: Jessica Kingsley Publishers. 1 For example, see the work of Heimann (1950), Bion (1970), Racker (1968) and Money-Kyrle (1956), as well as Joseph (1989), Segal (1981) and Rosenfeld (1965) among others. It may be helpful if I remind you that projective identification is based on the need to expel feelings and fantasies that are felt to be explosive and bad. It involves an attack on one’s external objects, and an attempt to control them. However, it also involves non-verbal communication. Thus, projective identification involves processes of expulsion, attack, control and non-verbal communication. These processes are governed by the repetition compulsion rooted in early traumatic experience. Malign projective identification should be distinguished from benign or at least nonmalign forms of it. The essence of benign projective identification is non-verbal and pre-verbal communication. This is ubiquitous in the transference of psychic reality, no matter in what phase of development the specific material originated, but it is the essence of the communication of pre-Oedipal experience. Introjective identification consists of unconscious processes that are reciprocal and complementary to those of projective identification. However, introjective identification can also 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 82 occur as the first step in the unconscious relationship. (I suppose that projective and introjective identification can occur with respect to one’s own internal objects as well, but this is a very complex matter, and not entirely relevant here.) It is not that the patient uses projective identification and the analyst uses introjective identification; the patient also uses processes of introjective identification, and the analyst, processes of projective identification. There are both malign and benign forms of introjective identification, just as there are both malign and benign forms of projective identification. For a thorough discussion of these processes see Scharff, J. (1992). 2 In this context, I can only mention the work of Fairbairn (1952), Winnicott (1956), Balint (1965), Bowlby (1982) and Khan (1963), and with regard to the next generation, the work of Bollas (1987), Casement (2002), and Pedder (1979), among many others. 3 I personally very much agree with the implicit emphasis on understanding the repetition compulsion in terms of very early traumatic experience rather than the so-called ‘death instinct’. Although I will return to the topic of traumatic experience and transference and countertransference processes, the more theoretical topic of the death instinct and the repetition compulsion is beyond the scope of the present enquiry. 4 Countertransference edited by Epstein and Feiner (1979) is an especially useful collection of papers about countertransference that reflects the development of the various debates as of the mid-1970’s. Also useful is Countertransference Analysis by König (1995), who is both a psychoanalyst and a group analyst. Key Papers on Countertransference edited by R. Michaels et al was published in 2002, and is a definitive statement to date. 5 An especially useful and balanced summary of the main tenets of the relational perspective is the new edition of The Power of Countertransference by Karen Maroda (2004). Juan Tubert- 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 83 Oklander (2003 and 2005) has written a series of important articles in which he synthesises relational work in the Kleinian tradition. 6 They range from Fromm (1956) and Horney (1945) to Fromm-Reichmann (1950), Sullivan (1964) and Thompson (1964). Although Langs (1976) and Searles (1979) led this revision in American psychoanalysis, the main contributors to it include Bacal (1998), Benjamin (1995), Greenberg and Mitchell (1983), Hoffman (1983), Levenson (1994), Mitchell (1988), Mitchell and Aron (1999) and Stolorow and Atwood (1992). 7 For example, in his discussions of the inauthentic interpretation Stewart (1987) quotes Herbert Rosenfeld, who ironically was one of the leading senior males in the field of Kleinian analysis, as saying: ‘If I hear one more student or one more colleague who is in a state of confusion about what is being said to him, who says to me in supervision that my patient has put his confusion into me, has shoved his confusion into me, or I am so angry with him for turning up late all the time, but it’s not my anger, it’s the anger that my patient is shoving into me, I am going to lose my mind’. In other words, an analyst who is anxious about feeling the feelings of another person and about being uncertain where those feelings originate, is likely to talk incessantly about having had feelings shoved into him; although this may be the case, a preoccupation with this suggests that the subtleties and complexities of the homosexual countertransference need to be analysed. However, in the light of the questions that I have raised about the meaning of the concept of interpretation, it will readily be seen that before offering an interpretation of a more scientific, classical kind, it is necessary first to make several different kinds of translation, e.g. to answer the question of why ‘shove’ means ‘bugger’, as opposed, or in addition to, ‘force feed’. 8 For example, see Freud (1915); Jung (1946); Sandler et al (1970); Blum (1973); Spector- Person (1985), to cite the work of only a few fairly classical psychoanalysts. 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 9 84 For example, see Meltzer (1974), Gorkin (1985), McDougall (1995), and Kernberg (1995), among many others who have examined the connections between the fully eroticised transference and borderline and narcissistic personality characteristics. 10 11 See the discussion of the theory and concept of the social unconscious in Appendix I. Of course, I am not Jung, and Jung is not here, and I always try to avoid analysing the content of a dream, preferring to focus on the analysis of the dreamer, because without the dreamer’s associations to the elements of a dream, you can only work in terms of your own associations to the manifest content of the dream; the latent content of a dream belongs to the dreamer, and we must be careful not to impose our own personal associations onto this. 12 Incidentally, I have not brought this quotation in order to offer a subtle comparison of psychoanalysis with Jungian analytical psychology; in any case, nowadays the analytical psychologists are much closer to the psychoanalysts than they once were. For example, both Jungians and Kleinians acknowledge the similarities between the concept of archetype and the concept of unconscious phantasy. 13 14 See my discussion of the social unconscious and the collective unconscious in Appendix I. As you know, at one stage in his work, primarily in connection with his discussions of sibling dynamics, Freud introduced the concept of the family complex in order to capture the importance of the non-biological nature of the Oedipus complex and its development. Unfortunately, psychoanalysts have not been able to appreciate the importance of the ‘family complex’, believing that they must emphasise the concept of the Oedipus complex based entirely on innate fantasy life. However, many group analysts have picked up this concept of the family complex because they have so much clinical experience of the repetition within a group of the full dimensions and variety of Oedipal configurations. I would remind you that from the point of view of group analysis, the Oedipus complex is not merely a matter of an innate biologically based fantasy of mother, father and infant and their various relationships; it is 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 85 also based on the form of the family, including sibling relationships, especially the sex of the siblings, place in the birth order, and number of years between siblings, and even the value that a particular community assigns to the birth of a boy or to being the first born, etc. In other words, The Oedipus complex involves fantasies and memories about all the relationships within the family of origin, and these fantasies and memories have a kind of natural history. 15 See the discussion of the theory and concept of the social unconscious in connection with the group as a whole in Appendix I. 16 There are several categories of models of group development and group regression: progressive models, cyclical models, and non-sequential models (Mennecke, Hoffer and Wynne, 1992). Most psychoanalytical models are progressive, but some are non-sequential. Not all progressive models are psychoanalytical models, for example, see the work of Agazarian (1997); Bennis and Shepard (1956); Budman et al (1996); Durkin (1981); MacKenzie (1997); MacKenzie and Livesley (1983); Rutan and Stone (2000); Schermer and Klein (1996); Silverstein (1997); Tuckman (1965); and Berman and Weinberg (1998). 17 I (Hopper 2003a and 2003b) have presented many cases of equivalence and their microcosms, based on my work on the foundation matrix and open systems theory connecting organisms, persons, groups and more complex social systems: 1) The co-creation of what the members of a group inside a larger organisation perceived to be the power structure and conflicts of their wider organisation. The National Health Service was perceived as father, the group as mother, and the group analyst as an ineffectual uncle. Part object splitting was involved. Kibel (2005) has also presented examples of group microcosms based on their equivalence with situations within the organisation in which a group was conducted. 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 2) 86 The co-creation of what the members of a group unconsciously imagined was the pattern of life that was typical of the Bajan village from which an AfroCaribbean member of the group originated. This process was an attempt to feel and to verbalise his painful emigration experiences as well as his troubled attempts to integrate into middle class English life (Hopper, 2003a, pp.164165). 3) The co-creation of what the members of a group unconsciously imagined was the small Welsh village in which one of its members lived during her infancy and childhood. The group formed a version of the class and status hierarchy in the village, and the men in the group began to relate to one another as though they were her father, her uncle and two of her brothers. I was regarded as her grandfather (Hopper, 2003a, pp. 126-161). 4) The co-creation of what a group of child survivors of Shoah atrocities unconsciously imagined was the atmosphere of a concentration camp in which most of their parents had been murdered. Similarly, Kreeger and I (Hopper, 2003a, pp. 72-94) have described the unconscious co-creation of the atmosphere of a death camp during a large group of participants in a Conference about the Survivor Syndrome. 5) The co-creation of what a group unconsciously imagined was the political life of the United States, partly as a displacement from their sense of what was going on in my mind during the run up to the Presidential Election . Similarly, a group of child survivors unconsciously co-created a warm and supportive way of life that they felt I needed in order to replace what I had lost from my childhood and earlier life in the United States. This group tried to become my 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 87 parents and my lost family in a way that allowed them to avoid recognising their pain at having lost their own parents (Hopper, 2003b, pp. 138-149). 6) The co-creation of what a group unconsciously imagined was the fragmentation of European society around the time that the Maastricht Treaty was signed (Hopper, 2003a pp. 144-145). Similarly, seminars in training courses often reproduce the dynamics of the organisations that sponsor and support the courses, including the atmosphere of the administrative office as well as that of the governing committees. Although I have not written about my experiences as a consultant to film directors and about film scripts and their productions, I have observed over and over again that the script and its central tensions resonate unconsciously among the actors and everyone else involved in making the film, very much like what is portrayed in The French Lieutenant’s Woman, based on John Fowles’ (1969) novel, or in Day for Night by Francois Truffaut (1973). In these cases it became very difficult to know who was expressing what for whom, and where the basic script was located, that is, in what matrix and at what level of communication. Of course, questions about ‘location’ are typical of group work of all kinds, but such questions were especially relevant in these attempts to produce films of scripts that were intermediary and transitional between the various groups and their members that were involved in the task. 18 It is another matter that unfortunately our profession is organised like a very large and complex church with many priestly orders, and that many psychoanalysts interpret their perceptions of the transference as though they were engaged in ritual prayer, which is a function of what Racker (1968) termed the ‘indirect countertransference’, in reference to the way that some analysts are overly influenced by their transference to their professional associations. 12/02/16 Notes for Lectures on the Concepts of Tr and Ctr in p-a, pgp and g-a 19 88 For example, in thinking about unconscious aspects of the so-called ‘national identity’ of Israelis as a people or of Palestinians as a people, I would use the concepts of the shared unconscious and of the interpersonal unconscious in order to describe and explain the role of the ‘projected other’, but I would not refer to either the social unconscious or the collective unconscious of Israel, Palestine or the Middle-East as a whole (Kelman, 1999).
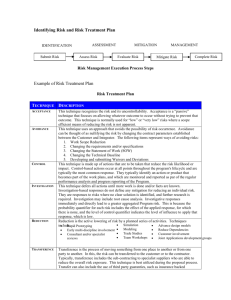
![UW2 - Psychiatric Treatments [2014]](http://s3.studylib.net/store/data/006859622_1-db6167287f6c6867e59a56494e37a7e7-300x300.png)