Diabetic Ketoacidosis (DKA) Admission From ED Orders
advertisement
 Admission From ED Orders")
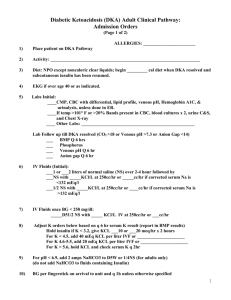
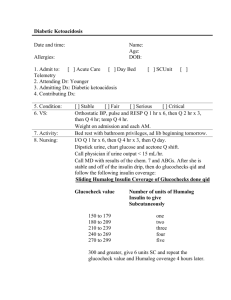
PLACE LABEL HERE DIABETIC KETOACIDOSIS (DKA) ADMISSION FROM ED ORDERS The following orders will be implemented. Orders with a “” are choices and are NOT implemented unless checked. Initial all handwritten order modifications and the bottom of each page when indicated (multipage). 1. Diagnosis & Status: Admit as Inpatient _________________________________________(reason for admission) 2. 3. Mild diabetic ketoacidosis: CO2 equal to 21 to 28 mEq/L and /or pH 7.3 Moderate diabetic ketoacidosis: CO2 equal to 11 to 20 mEq/L and/or pH 7.1 to 7.3 Severe diabetic ketoacidosis (ICU recommended): CO2< 10 mEq/L and/or venous plasma pH< 7.1 Hyperosmolar Hyperglycemic State (HHS) (ICU recommended) is characterized by severe dehydration, with absent or small ketones. This pre-printed order can be used with modifications for patients with HHS. Unit: ICU IMCU/PCU Consults: __________________________________________________________________________ Consult Diabetes Educator and Clinical Dietitian 4. 5. 6. 7. 8. 9. 10. Diagnostics/Lab : BMP magnesium, and phosphorous on admission to unit if not done in ED BMP q 4 hrs x 2, then q 6 hrs x 4 HbA1C if not done in ED CBC, CMP q AM Serum hCG, for females 10-60 years of age, if no pregnancy test done in ED Serum ketones q hrs x ________ Radiology: _______________________________________________________ Other: ___________________________________________________________ Vital signs per unit routine Urinary Retention Orders (form # 31620), initiate if patient has urinary retention or difficulty voiding Activity: Bedrest BSC BRP Up ad lib Oxygen per Respiratory Care Protocol (policy #7500-10-01-03) Adjust O2 to maintain SpO2 > 90% or 88% in COPD. Call physician for O2 usage > 4 L/min or > 40%. Reassess daily, wean O2 to maintain SpO2 > 90% or 88% in COPD. Wean to room air if SpO2 is acceptable and patient has no known exclusions per 7504-10-01-03. May restart O2 as needed. Post op patients will be weaned to room air the morning following surgery unless SpO2 is < 90% (88% for COPD) or patient has other exclusions. Cardiac monitoring: May be off monitor for testing Diet: NPO, when anion gap is < 13 advance to clear liquids If patient tolerates clear liquids, call physician for SQ insulin orders (form # 20383) Advance to consistent carbohydrate diet when subcutaneous insulin is initiated MEDICATIONS: 11. 12. Initiate or continue insulin infusion (use IV infusion pump) using the following: Regular insulin 100 units in NS 100 ml (1 unit/ml concentration) Start insulin infusion at rate determined by: (BG – 60) X 0.03 = number of units insulin/hour (BG = current blood glucose; 0.03 is the “multiplier”) Send copy to pharmacy *3-24148* Order writer’s Initials___________ FORM 3-24148 REV. 06/2012 Page 1 of 2 PLACE LABEL HERE DIABETIC KETOACIDOSIS (DKA) ADMISSSION FROM ED ORDERS 13. Finger stick blood glucose (BG) check q 1 hr until BG within 100-150 x 3 readings, then q 2 hrs The following orders will be implemented. Orders with a “” are choices and are NOT implemented unless checked. Initial all handwritten order modifications and the bottom of each page when indicated (multipage). 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. With subsequent hourly glucose checks, adjust multiplier in formula using the following directions: BG is < 100 decrease multiplier by 0.01 BG is 100 – 150 no change in multiplier and recalculate infusion rate BG is > 150 increase multiplier by 0.01 Do not stop insulin infusion for NPO status Blood glucose (BG) < 60 mg/dL: initiate Hypoglycemia Protocol (form # 2513). Stop insulin infusion. Recheck BG q 15 min until BG > 100mg/dL then restart insulin infusion at ½ previous rate. IV Fluids for blood glucose over 250 mg/dL: NS with KCL 20 mEq/L IV at ______ ml/hr for ______ liters, then ½ NS with KCL 20 mEq/L IV at _________ ml/hr for ________ liters LR at __________ ml/hr IV Fluids for blood glucose less than or equal to 250 mg/dL: D5 ½ NS IV at __________ ml/hr x 1 liter D5 NS IV at ____________ ml/hr x 1 liter D5 ½ NS with KCL 20 mEq/L IV at _________ ml/hr x 1 liter D5 NS with KCL 20 mEq/L IV at _________ ml/hr x 1 liter Magnesium (Mg++) less than 1.8: Magnesium sulfate 2 gm IV over ________ hr(s) Recheck Mg ++ after infusion completed and repeat prn if Mg ++ less than 1.8 Potassium (K) less than or equal to 4.0: KCL ____ mEq IV over _____ hr(s), Recheck K after infusion completed, repeat prn if K < 3.3 KCL 40 mEq po now x 1 dose Potassium > 5: delete potassium from maintenance IV and check potassium q 2 hrs Stress ulcer prophylaxis: Pepcid (famotidine) 20 mg IV or po twice a day DVT prophylaxis: Lovenox (enoxaparin) 40 mg SQ q day at 1700, if CrCl < 30, 30 mg SQ q 24 hrs Antiembolitic compression hose Foot pumps PRN MEDICATIONS (If > one drug is ordered for the same indication, clinical assessment will be used per policy 520-06) 24. Mild pain/temp >100.5F/HA: Tylenol (acetamino 25. Nausea/vomiting: Zofran (ondansetron) 4 mg IV q 6 hrs prn Reglan (metoclopramide) 10 mg po or IV q 6 hrs prn (5 mg if > 65 y/o) Phenergan (promethazine) 12.5-25 mg po or per rectum q 4 hrs prn 26. Constipation: Ducolax 10 mg per rectum daily prn ADDITIONAL ORDERS: ______________________________________________________________________________________ ______________________________________________________________________________________ ______________________________________________________________________________________ ______________ Date ___________________ Time _________________________________ Physician Signature ___________ PID Number Send copy to pharmacy FORM 3-24148 REV. 06/2012 Page 2 of 2