DI-Chest-Lung Ca

RADIOLOGY CASE REPORT
Patient ID: OH# 22417802
Type of Study: Chest Radiograph, PA and Lateral
Date of Study: August 6, 2008
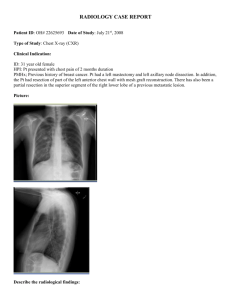
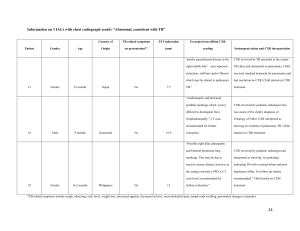
1. Clinical Indication: 79 yo female. History of Carcinoma. Increased confusion, increased white blood count and history of weight loss. Comparison: None available.
2. Picture:
2
2. Describe the radiological findings:
In Right lung field there is a small right pleural effusion. There is an area of consolidation in the right upper lobe with associated bronchiectasis. There is partial collapse of the right upper lobe with signs of right lung volume loss. Note the elevation of the right hemidiaphragm. The minor fissure is pulled upwards and forms a reverse S configuration representing the “reverse S Golden sign”. The cardiac contours are within normal limits. The bony thorax is unremarkable. There is no tracheal shift.
Findings: pleural effusion, consolidation, bronchiectasis
Impression: Right upper lobe consolidation with partial collapse and distal bronchiectasis. According to radiologist, this is very suggestive of an underlying right hilar cancer.
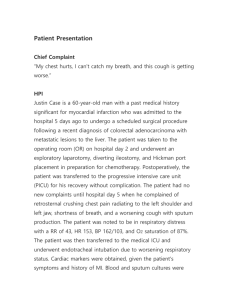
The Golden S sign can be seen on posteroanterior chest radiographs of right upper lobe collapse when a large enough central mass is present to produce a downward convexity of the medial or proximal portion of the minor fissure.
Note above the convexity * from the mass and the concavity ** of the minor fissure.
3. Provide possible diagnosis(es):
The major abnormality is right upper lobe/right middle lobe mass. Can be a benign or malignant tumor. The Golden S sign is created by a central mass and should raise suspicion of a central neoplasm, such as primary bronchial carcinoma. 80 % of lung cancers are non–small cell lung carcinomas, which include adenocarcinoma, squamous cell carcinoma, and large cell carcinoma. Other central masses to consider include metastasis, primary mediastinal tumor, or enlarged lymph nodes. However, sometimes patterns of upper lobe collapse can result in an apparent Golden S sign in the
3 absence of a mass.
Although bronchogenic carcinoma cannot be dx definitively on the basis the Golden S, this sign should be recognized and should alert the radiologist to consider the diagnosis.
Note: A CT thorax with contrast was done the following day of the above chest x-ray and changes within the right lower lobe were suggestive of lymphangitic carcinomatosis.
_____________________________________________________________
4. What would you recommend next for this patient?
CT scan or MRI may provide more precise information about the possibility, size, shape, and location of any tumors. Chest CT scan with contrast would be a good choice for this patient along with FLUOROSCOPIC GUIDED LUNG BIOPSY of the RUL.
________________________________________________________________________
5. Is the use of this test/procedure appropriate?
Plain chest radiography is the initial investigation of choice in patients presenting with any respiratory symptoms, and this examination is used in staging most cancers.
However, the sensitivity of chest radiography in the detection of lymphangitic carcinomatosis (LC) is only approximately 25%. Based on this patient’s age, history of carcinoma and weight loss along with increased confusion and increased white blood count, I would say that chest x-ray was very appropriate.
________________________________________________________________________
6. Is(are) there any alternate test(s)?
In the appropriate clinical circumstances or when the chest radiographic findings are equivocal, the next investigation employs high-resolution computed tomography (HRCT) scanning. Although the appearance of LC on HRCT scans is nonspecific, the observation
of certain features in a symptomatic patient with an appropriate history of malignancy is
4 highly suggestive of LC.
________________________________________________________________________
7. How would you explain to the patient about the possible risks and benefits of this test?
Benefits-
If a picture is worth a thousand words, the images from a CXR can be invaluable in detecting problems with the heart or lungs. CXR can offer a lot of info. about the patient’s health for little risk and expense. Quick and easy procedure and it is particularly useful in emergency dx and treatment.
Patient can have a series of CXR over time for comparison. No radiation remains in a patient's body after an x-ray examination. X-rays usually have no side effects in the diagnostic range.
Risks-
Patient’s may be concerned about radiation exposure from CXR, especially if they have them regularly. There is always a slight chance of cancer from excessive exposure to radiation. However, the benefit of an accurate dx far outweighs the risk.
The amount of radiation from a CXR is low. The effective radiation dose from this procedure is about 0.1 mSv, which is about the same as the average person receives from background radiation (eg. radon from rocks and soil) in 10 days. In addition, care is taken during X-rays to minimize what small exposure the patient does have. The smallest possible dose of radiation is used.
________________________________________________________________________
8. What is the cost of this test?
The estimated cost of a CXR is $50 to $80. The cost of a serial CXR is about $110 http://www.enlmedical.com/article/003804.htm
The cost can vary depending on the centre. The combined cost for PA and lateral chest radiographs and the radiologist's report can possible cost up to $500. Some hospitals have a certain budget, especially rural, and they pay a certain amount per year for the technical aspect of things.
________________________________________________________________________