Berkshire West FH Information Pack
advertisement

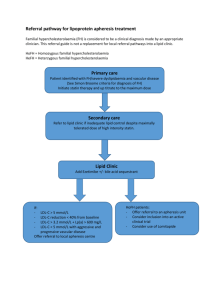
Berkshire West FH Information Pack Familial Hypercholesterolaemia (FH) cascade testing patient pathway in Berkshire West Patient visits GP – routine blood test indicating high lipids. Patient already on statins. Calculate pre LDL level as per table in pathology handbook via Webpath Concern about FH based on family history Check family history for early death from CVD and perform fasting lipid profile. If LDL cholesterol > 5.5 mmol/l and triglyceride < 2.0 mmol/l and preferably there is a family history of MI before age of 50 in 2nd degree relative or before age of 60 in 1st degree relative If triglyceride ≥ 2.0 mmol/l treat as usual with statin. Give lifestyle advice and refer to weight management and physical activity services as appropriate GP appointment required GP Actions: GP and patient discuss FH. Give lifestyle advice and refer to weight management and physical activity services as appropriate. Inform patient they are being referred to Lipidologist and give patient information leaflet (appendix 5). Complete virtual clinic proforma available on Choose and Book to refer to virtual lipid clinic. Commence /continue to treat with statin as per protocol (appendix 3/4) Lipidologist will decide on genetic testing based on information provided in pro- forma. Decision not to test: Lipidologist will write to GP with further advice. Decision to test: Lipidologist writes to patient, enclosing blood test form advising patient to go their GP practice to have the blood test done. Informative letter sent to GP If test positive: Informative letter sent to GP. Lipidologist If test negative will write to patient to communicate positive result and refers patient to FH co-ordinator who will start cascade testing for family members . Lipidologist will write to inform patient and GP of result and treatment recommendations. Below this point, pathway to be mainly actioned by Lipidologist & FH Co-ordinator if patient tests positive LDL-C Correction Factor Table for patients on cholesterol lowering medication If untreated LDL-C levels are unobtainable, then the following table can be used to estimate untreated values. To achieve this, multiply the treated LDL-C value by the appropriate correction factor. Statin / dose (mg) Correction Factor Ezetimibe 10 Pravastatin 1.2 10 20 40 1.2 1.3 1.5 Pravastatin + Ezetimibe 10 + 10 20 + 10 40 + 10 1.5 1.6 1.7 Simvastatin 10 20 40 80 1.4 1.6 1.7 1.9 Simvastatin + Ezetemibe 10 + 10 20 + 10 40 + 10 80 + 10 1.9 2.0 2.3 2.4 Atorvastatin 10 20 40 80 1.6 1.8 2 2.2 Atorvastatin + Ezetemibe 10 + 10 20 + 10 40 + 10 80 + 10 2 2.2 2.2 2.5 Rosuvastatin 5 10 20 40 1.8 1.9 2.1 2.4 Rosuvastatin + Ezetimibe 10 + 10 20 + 10 40 + 10 2.5 2.7 3.3 Treatment with Atorvastatin For patients with Familial Hypercholesterolaemia, aim for more than 50% LDL-cholesterol reduction from baseline. Ideally, LDL-cholesterol should be <2.5 mmol/L In general, 40 mg od or higher doses of Atorvastatin will be needed to reduce LDL-cholesterol to target but note that some patients may develop myalgia and may need a different statin. Should this be the case, we suggest that rosuvastatin (starting with a dose of 5 mg od) is tried first as this statin appears to be better tolerated than simvastatin. Pravastatin is a very weak statin and should only be tried if other statins cause side-effects. Start with Atorvastatin 40 mg od. After 8 weeks, repeat fasting lipid profile. If LDL-cholesterol, has not achieved 50% reduction from baseline, double the dose of atorvastatin to 80 mg od. If using rosuvastatin, double the dose too. Suggest measure ALT at this stage to rule out liver damage. Repeat fasting lipid profile 8 weeks later. If Atorvastatin 80 mg od has not lowered LDL-cholesterol to target, add ezetimibe 10 mg. An alternative is to use rosuvastatin at 40 mg od +/- ezetimibe. Other drugs that can be used in combination with statins to achieve LDL-cholesterol target are: Fibrates: suggest use fenofibrate 200 mg od. Be cautious when combining atorvastatin 80 mg od and fenofibrate 267 mg od due to relatively high risk of myalgia/myositis (this is due to prolonged half-life of atorvastatin). Weight and physical activity interventions Tiers of weight management Tier 1 (BMI 25 – 29.5) Walk-in4health BMI/Referral pathway/criteria Name of the service/provider Venue/costs/booking BMI 25 onwards Flexible for high risk groups like Asians & African Caribbean groups Weight Management Team, Public Health, West Berkshire Council Market Street Newbury RG14 5LD Reading walk-in centre, Broad Street Mall, Reading –FREE Drop-in service, selfreferral; can be referred by a professional as well Eat4health BMI 25 onwards Flexible for high risk groups like Asians & African Caribbean groups Self-referral Referral through GP/HCP for those with comorbidities/risk factors Healthy lifestyle information Health walks, lifestyle interventions (varied) Monday 10.30-12.00 & Thursday 11am-12.30 Men Only £3.90: Friday: 6.30pm-8pm) Weight Management Team, Public Health, West Berkshire Council Market Street Newbury RG14 5LD Leisure centres/community venues/ GP surgeries Reading Borough Council Bookings: mbenford@westberks.gov.uk 01635 503410 Runs across Reading (7), West Berkshire (6) and Wokingham (3) in a total of 16 venues. It has been part of the NICE call for evidence and proven successful since the past 3-4 years Cost per course: £3.75 FREE vouchers available for people on benefits and low income Bookings: mbenford@westberks.gov.uk 01635 503410 Reading From GP desktop http://nww.berkshirewest pct.nhs.uk/page.asp?fldA rea=5&fldMenu=16&fld SubMenu=0&fldKey=16 36 Reading Lifestyle Interventions Sport Reading Information Pack. Contact Sport Reading on 0118 9015713 or visit their website at www.sportreading.co.uk West Berkshire West Berkshire council West Berkshire Lifestyle Interventions Activity for Health Scheme Contact 01635 31199 Wokingham Wokingham council Wokingham Lifestyle Interventions Wokingham Borough Council’s Health and Physical Activity Initiatives. Active Wokingham’s GP Exercise Referral Scheme and referral criteria Wokingham Contact 0118 9746264 Tier 2(BMI => 30-35) Eat4health BMI 25 onwards (Flexible for high risk groups like Asians & African Caribbean groups) Weight Management team, Public Health, West Berkshire Council Market Street Newbury Runs across Reading (7), West Berkshire (6) and Wokingham (3) in a total of 16 venues. It has been part of the NICE call for evidence and proven successful since the past 3-4 years Patient Information leaflet Familial Hypercholesterolaemia Familial hypercholesterolaemia is an inherited condition, in which the level of low-density lipoprotein (LDL) cholesterol in the blood is higher than normal from birth. The condition may be discovered if you have a routine health check. Or, you may notice some of the features such as fatty lumps on the skin or around the eyes. Treatment includes living healthily and taking medicines to keep the cholesterol level down. What is familial hypercholesterolaemia? Familial hypercholesterolaemia is a term applied to an inherited condition in which low-density (LDL) cholesterol (often referred to as bad cholesterol) is at a higher than normal level in the blood. See separate leaflet called 'Cholesterol' for more information about cholesterol and the different types of cholesterol. What causes familial hypercholesterolaemia? Familial hypercholesterolaemia is caused by a defect in a gene which controls the way cholesterol is handled in the body. As a result of the defect, LDL cholesterol is not broken down properly and builds up in the bloodstream. In most cases the defective gene is inherited from one parent (heterozygous inheritance). If you inherit it from both parents (homozygous inheritance), the condition is more severe. Heterozygous familial hypercholesterolaemia affects about 1 in 500 people. The homozygous condition is rare. What are the features of familial hypercholesterolaemia The most important feature is the development of heart disease at a young age. This is caused by plaques of atheroma developing within the walls of the coronary (heart) arteries (see below). This can lead to a heart attack (myocardial infarction) as a young adult. You might also notice: Xanthomas - fatty cholesterol-rich deposits in the skin, usually found around the elbows, knees, buttocks and tendons. Xanthelasmas - fatty deposits in the eyelids. Arcus senilis - a white ring around the cornea (the coloured part of the eye). Obesity. What are atheroma and cardiovascular diseases? Patches of atheroma are like small fatty lumps that develop within the inside lining of arteries (blood vessels). Atheroma is also known as atherosclerosis and hardening of the arteries. Patches of atheroma are often called plaques of atheroma. A main risk factor for developing atheroma is a high blood cholesterol level. Over months or years patches of atheroma can become larger and thicker. So, in time, a patch of atheroma can make an artery narrower. This can reduce the blood flow through the artery. For example, narrowing of the coronary (heart) arteries with atheroma is the cause of angina. Sometimes a blood clot (thrombosis) forms over a patch of atheroma and completely blocks the blood flow. Depending on the artery affected, this can cause a heart attack, a stroke, or other serious problems. Cardiovascular diseases are diseases of the heart muscle or blood vessels. When doctors say cardiovascular disease they usually mean diseases of the heart or blood vessels that are caused by atheroma. In summary, cardiovascular diseases that can be caused by atheroma include: angina, heart attack, stroke, transient ischaemic attack (TIA, or mini-stroke), and peripheral vascular disease. In the UK, cardiovascular diseases are a major cause of poor health, and the most common cause of death. How is familial hypercholesterolaemia diagnosed? You may be diagnosed by chance if you go for a health screening check or you may notice fatty deposits on the skin or around the eyes. Another member of your family may be diagnosed with familial hypercholesterolaemia or have a heart attack before the age of 50, and you may be advised to have a check yourself. You will be advised to have a blood test to check your cholesterol. Familial hypercholesterolaemia is suspected in adults if the total cholesterol is 7.5 mmol/L or greater, or the LDL cholesterol is 4.9 mmol/L or greater. In children (between the ages of 10 and 15) the levels are 6.7 mmol/L and 4.0 mmol/L respectively. What are the aims of treatment? You are unlikely to have any symptoms from the heterozygous (less severe) form of familial hypercholesterolaemia as a child or young adult. However, you should be treated to stop symptoms and complications from developing when you are older - the most important of which is heart disease that may develop at an earlier age than usual. What are the treatment options for familial hypercholesterolaemia? Being a genetic disorder, familial hypercholesterolaemia is not caused by an unhealthy lifestyle. However, keeping yourself in the best physical condition will help to prevent future problems. Things you can do to help yourself include: Eating healthily - you will almost certainly be referred to a dietician to help you with this, even if you are not overweight. Getting a reasonable amount of exercise. Avoiding smoking. Maintaining a normal weight. You will be offered medication to help bring your cholesterol level down. The usual medicine to start with is a statin. The most common statin used is called simvastatin. If the level does not come down, another medicine called ezetimibe is sometimes added. Affected children usually start statin medication in late childhood or early adolescence. Some children may need apheresis (a treatment which filters LDL cholesterol out of the blood). This is offered to those who have the greatest risk of developing problems. In particular, those with the rare homozygous form of familial hypercholesterolaemia. Your GP may want to discuss referring you to a specialist. A specialist can advise about your treatment and arrange the testing of close members of your family. What is the outlook (prognosis)? The outlook for people with heterozygous familial hypercholesterolaemia is usually good if you maintain a healthy lifestyle, have regular checks and take your medication without fail. The most significant complication is heart disease or another cardiovascular disease that may develop at a younger age than usual. The outlook for those with the more severe (homozygous) form of the condition is less good.