Anticoagulation Clinic Guidelines
advertisement

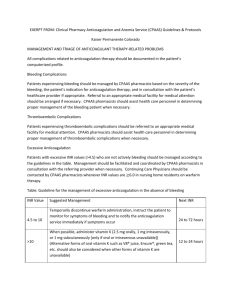
Anticoagulation Clinic Guidelines (Draft) Dean Medical Center The Anticoagulation Clinic(AC Clinic) is a service staffed by pharmacists and nurses with specific knowledge in anticoagulation therapy. Anticoagulation care is managed under the supervision of the AC Clinic Medical Director and the patient’s physician. I. Goals and Objectives A. To provide services to physicians initiating anticoagulation therapy and assist physicians in the management of oral and parenteral anticoagulants. B. To provide consistent management and follow-up care for patients receiving anticoagulation therapy by evaluating patient-specific data and pertinent laboratory tests dependent upon the anticoagulant regimen. C. To provide consistent education to the patient and/or family members about warfarin and other anticoagulant therapy. To make them aware of potential problems during therapy and the signs and symptoms of bleeding, embolic events and other adverse effects. D. To consistently identify patients who are non-adherent with the anticoagulation care plan and provide education to improve adherence and reduce the potential for adverse events and maximize the benefits of treatment. . E. To maintain an anticoagulation flowsheet for each patient and provide complete documentation of the care provided in the patient’s electronic medical record. F. To consult with other providers involved with the patient’s care when needed. II. Scope of Care A. Patient Referral 1. Patients may be referred to the AC Clinic if they have demonstrated the capability to self-administer medication, or have a responsible caregiver who can supervise the medication administration, or other acceptable process in place to ensure adherence to the treatment plan. A reliable method of communication must exist for the patient to be enrolled in the AC Clinic. The AC Clinic is unable to manage the patients with the following issues: a. uncontrolled alcohol abuse b. underlying psychiatric problems hindering adherence to program expectations c. inability to adhere to care plan d. patients with no reliable means of communication 2. Patients may be referred to the AC Clinic at any point during anticoagulation therapy provided that a collaborative care agreement exists between the AC Clinic and the supervising physician (See below: Collaborative Care Agreement). The patient must be assessed by the supervising physician periodically to determine need for further anticoagulation therapy. 1 Dean Anticoagulation Clinics COLLABORATIVE CARE AGREEMENT I, __________________________________ MD / DO, acknowledge that I have read and approve the Guidelines of the Dean Anticoagulation Clinics (AC Clinic). My signature on this document authorizes the AC Clinic clinician to monitor my patients’ anticoagulation therapy. This collaborative agreement may be terminated at any time for an individual patient either by me or the AC Clinic clinician for any reason including: anticoagulation therapy is discontinued, patient desires to be followed by the primary physician alone, or the patient misses 3 consecutive appointments, blood draws or other laboratory test used to maintain control of the anticoagulation therapy without contacting the AC Clinic staff. Check all of the following that apply: ___ It is not necessary for the AC Clinic clinician to call me for routine changes in therapy. ___ The AC Clinic clinician may authorize prescriptions for warfarin to the patient’s pharmacy on my behalf. Physician’s Signature___________________________________ Date_______________ Please print name____________________________________________________________ 2 4. Referrals to the AC Clinic can be made by the primary physician verbally, by electronic referral, or by written orders. The referral should indicate the reason for use, desired intensity of treatment, and planned length of treatment. If the physician has already prescribed a dosage of the anticoagulant, the strength of medication and dosage per day needs to be indicated. 5. The AC Clinic will establish a computerized patient file for each new referral. After reviewing the patient’s medical record, the AC Clinic clinician will complete a initiation form in Epic. The patient’s medical record will be evaluated to obtain the information listed below. If not specified by the primary physician, the desired INR range will be based on the current American College of Chest Physicians Consensus Conference guidelines for the specific indication along with individual patient characteristics. The AC Clinic clinician will contact the physician, when needed, to determine the target range and duration of treatment for the intended therapy. The AC clinician will provide the physician the literature recommendations for usual target range and duration of therapy for the specified indication, if needed. The computerized medical record should have the following information available to the AC Clinic clinician for review: a. patient name, address and telephone number (home/work) b. emergency notification contact (telephone number home/work) c. date of birth, weight, height, gender d. current medications, including prescription and nonprescription e. medical history: known diseases and surgeries, drug allergies and reactions, conditions relating current medication regimen, surgical history, and hospitalizations. f. indication for anticoagulation therapy g. target INR range and planned duration of therapy h. if already receiving anticoagulation therapy include: start date, current dose i. history of bleeding including major and minor (dates and outcomes) j. physician name, direct office telephone number, pager number, and fax number 3 Dean Anticoagulation Clinics INDICATIONS AND THERAPEUTIC RANGES Unless the desired INR range is specified by the primary physician on the patient referral form, the AC Clinic will use ranges for the corresponding indications below as recommended by the Commitee on Antithrombotic Therapy of the American College of Chest Physicians. INDICATION TARGET INR (RANGE) DURATION COMMENT Atrial Fibrillation (AF) Age < 65 no risk factors Age < 65 with risk factors for stroke (Hx TIA/stroke/TE; HTN, CHF, LV fxn; rheumatic mitral valve dz; valve replacement; DM; CAD; thyrotoxicosis Age 65-75 no risk factors Age 65-75 with risk factors Age > 75 Precardioversion (AF/flutter > 48 hrs in duration Postcardioversion (in NSR) None 2.5 (2.0-3.0) Chronic Chronic Aspirin alone 2.5 (2.0-3.0) 2.5 (2.0-3.0) 2.5 (2.0-3.0) 2.5 (2.0-3.0) 2.5 (2.0-3.0) Chronic Chronic Chronic 3 weeks 4 weeks Or Aspirin 2.5 (2.0-3.0) Chronic 2.5 (2.0-3.0) Chronic 2.5 (2.0-3.0) 2.5 (2.0-3.0) 2.5 (2.0-3.0) Chronic 3 months Chronic 2.5 (2.0-3.0) 2.5 (2.0-3.0) 3 months 3 months 2.5 (2.0-3.0) Chronic 2.5 (2.0-3.0) 2.5 (2.0-3.0) 2.5 (2.0-3.0) 3-6 months 6 months Chronic 3.0 (2.5-3.5) 2.5 (2.0-3.0) Chronic Chronic Weekly INRs Add antiplatelet Rx Cardioembolic Stroke With risk factors for stroke (AF;CHF;LV dysfxn; mural thrombus; Hx TIA/Stroke.TE) Following embolic event despite therapeutic anticoagulation Left Ventricular Dysfunction Ejection fraction <30% Transient, following myocardial infarction Following embolic event despite therapeutic anticoagulation Add antiplatelet Rx Acute Myocardial Infarction (MI) Following anterior MI Following inferior MI with transient risks (AF; CHF; LV dysfxn; mural thrombus, Hx TE) Following initial tx with persistent risks Thromboembolism (DVT,PE) Treatment/prevention of recurrence Transient risk factors Idiopathic Presisitent risk factors (AT-III; protein C; protein S deficiencies; Factor V Leiden; malignancy Antiphospholipid antibody syndrome Following recurrent DVT/PE 4 May need higher range Valvular Disease Aortic valve disease with mitral valve disease; AF; Hx systemic embolization Mitral annular calcification with AF; Hx systemic embolization Mitral valve prolapse: With AF; Hx systemic embolization With Hx of TIA despite ASA Rx S/p embolic event despite anticoagulation Rheumatic mitral valve disease With AF; Hx systemic embolization; LA > 5.5cm S/p embolic event despite anticoagulation 2.5 (2.0-3.0) Chronic 2.5 (2.0-3.0) Chronic 2.5 (2.0-3.0) 2.5 (2.0-3.0) 2.5 (2.0-3.0) Chronic Chronic Chronic 2.5 (2.0-3.0) Chronic 2.5 (2.0-3.0) Chronic Add antiplatelet Rx 2.5 (2.0-3.0) 2.5 (2.0-3.0) 2.5 (2.0-3.0) 2.5 (2.0-3.0) 2.5 (2.0-3.0) 3 months >3 months 3-12 months Chronic Chronic Followed by aspirin Rx Followed by aspirin Rx Followed by aspirin Rx 2.5 (2.0-3.0) 3.0 (2.5-3.5) 3.0 (2.5-3.5) 3.0 (2.5-3.5) 3.0 (2.5-3.5) 3.0 (2.5-3.5) 3.0 (2.5-3.5) 3.0 (2.5-3.5) 3.0 (2.5-3.5) Chronic Chronic Chronic Chronic Chronic Chronic Chronic Chronic Chronic Add antiplatelet Rx Valve Replacement-Bioprosthetic Aortic or mitral with LA thrombus with Hx systemic embolism with AF Following systemic embolism Add aspirin Rx Valve Replacement – Mechanical Aortic Bileaflet In NSR, normal EF, normal LA size All others Tilting disk Ball and cage Mitral Bileaflet Tilting disk Ball and cage With additional risk factors or following TE * 2.0-3.0 + aspirin81mg * 2.0-3.0 + aspirin81mg With aspirin * 2.0-3.0 + aspirin81mg * 2.0-3.0 + aspirin81mg With aspirin Add aspirin *In patients with risks for hemorrhage. Hx, history; TIA transient ischemic attack; TE, thromboembolism; HTN, hypertension; CHF, congestive heart failure; , lowered; LV left ventricular; fxn, function; dysfxn, dysfunction; dx, disease; CAD, coronary artery disease; AF, atrial fibrillation; NSR, normal sinus rhythm; MI myocardial infarction; tx, treatment; DVT, deep venous thrombosis; PE pulmonary embolism; s/p, status post; LA, left atrium; EF, ejection fraction 5 6. All referrals to the AC Clinic must have a supervising Dean Medical Center physician who is responsible for periodically assessing the patient’s continuing need for anticoagulation therapy and management of medical/surgical problems. 7. If difficulties arise, such as, lack of cooperation, continued non-adherence with INR blood draws, the primary physician will be made aware of the issues by the AC Clinic clinician. A note will be placed in the patient’s medical record describing the problem, discussion with the primary physician, and agreed upon course of action. If the issue continues to be problematic despite repeated efforts to rectify the problem, the patient may be referred back to the primary physician for reevaluation. 8. In addition to adherence issues, the AC Clinic clinician will notify or, if needed, refer the patient back to the primary physician or proceed to the hospital ER in the following circumstances: a. consultation with a physician is requested by the patient b. the AC Clinic clinician notes findings suggestive of another worsening medical problem c. there is evidence suggestive of gross hematuria, gastrointestinal, or other bleeding d. there is evidence suggestive of worsening thromboembolic disease e. assessment of continuing need for anticoagulation is warranted 9. Discontinuation of anticoagulation therapy will only occur by physician order. When the desired length of treatment has been reached, the the AC Clinic clinician will refer the patient back to the primary physician to evaluate the need for continued anticoagulation. Discharge from the AC Clinic will occur by physician order when: a. anticoagulation therapy is discontinued b. the patient desires primary physician to manage anticoagulation c. the primary physician decides to manage anticoagulation d. the patient violates adherence policy (see B.3) 10. The AC Clinic clinician must provide consultation only with the patient via an inclinic appointment, the telephone, US mail or MyChart. The AC Clinic clinician can leave a message on the patient’s voice mail or answering machine or speak with a family member, activated power of attorney for healthcare, or other designated person provided that the patient completes and signs the AC Clinic verbal permission form (see below). The completed and signed formed must be scanned into Epic by Medical Records. 6 PERMISSION FOR VERBAL COMMUNICATIONS (print name of patient or place patient label here) (birthdate) (street address) (city, state, zip code) (phone number) I permit Dean Health Systems, Inc. Anticoagulation (AC) Clinic personnel (“Health Care Providers”) to leave information regarding ongoing anticoagulation therapy on my voice mail or answering machine. In addition this authorization allows the AC personnel to discuss health information, in person or by telephone with the following family members or friends involved in my medical care: (List family members/friends and state the person’s relationship to the patient). Name Phone Number Relationship 1. 2. 3. 4. Patient’s Signature: Date: If this Release is signed by a representative on behalf of the patient, complete the following: Representative’s Name: Relationship to Patient: If, at any time, I do not want this information to be left on my answering machine or I want to change the names of the people listed above, I must notify the Anticoagulation (AC) clinic: by telephone at 608-252-8060, or by mail at the address listed below, or in person at the Anticoagulation Clinic at Dean Clinic. INSTRUCTIONS: Please sign this form and send to the following location: Dean Clinic Attention: Anticoagulation Clinic 1313 Fish Hatchery Road Madison, WI 53715 \\dhs\dfs\Groups\Pharmacy\Administration\Web Page\Anticoagulation Clinic\AC Verbal Permission form.doc 7 Rev 1/28/09 B. Clinic Procedures - AC Clinics: For Dean Fish Hatchery Road AC Clinics see visio below; For Riverview and Stoughton AC Clinic, see attached guidelines. 8 9 10 11 12 13 1. Patients will schedule appointments to the AC Clinic during regular office hours. The patient will be scheduled by the AC Clinic in Epic. The AC Clinic clinician will see patients as follow-ups, accept new consults and phone patients with INR results and changes in the care plan. Hospital patients who are enrolled after discharge need to be scheduled within 1 week of discharge. 2. For patient who are managed primarily by phone, they may have INRs drawn at any Dean Medical Center Laboratory, any outlying laboratory, via Home Health Service, or via point of care self testing. INR test results must be transmitted to the AC Clinic. When possible a hard copy from outlying laboratories will be scanned into Epic by Medical Records. Patients with inclinic appointments with the AC Clinic need toarrive at the Fish Hatchery Clinic Lab 1 hour prior to their appointment for their INR draw. They need to check in for the appointment at the appointment desk, then be seated at the AC Clinic Office area. If a patient can not attend a scheduled AC Clinic visit or have blood drawn on the day arranged the patient needs to call the AC Clinic to reschedule. 3. Missed appointments (no shows) – AC Clinic dismissal process a. AC Clinic Current No Show Process __Date________ __Available INR Reminder Notification_ __Documentation_ INR DUE (Day X) NO NO NO X+7 NO REMINDER CALL #1 FLOWSHEET/EXCEL X+14 NO REMINDER CALL #2 FLOWSHEET/EXCEL X+21 NO REMINDER CALL #3 FLOWSHEET/EXCEL X+28 NO REMINDER LETTER FLOWSHEET/EXCEL X+35 NO AC PROVIDER** YES (AC ROVIDER) **Per agreement with the Primary Care Leadership at Dean Clinic with the Dean Anticoagulation Clinics in 2011: non adherent patients, who have fully progressed through the process outlined above, will be sent back to their PCP to reassess the appropriateness of continued anticoagulation. If the patient is thought to be best served by anticoagulation, the AC Clinic would consider resuming care if the patient agreed to be compliant (that is, after the PCP has discussed the potential "second chance" with the patient). If during this “second chance” with the AC Clinic, the patient remains non adherent with their recommendations, the AC Clinic would not continue to monitor further anticoagulation therapy . The AC Clinic will inform the PCP of this action. The PCP will need to make the clinical judgment about further treatment and, if continued, the PCP would manage the anticoagulation therapy. FLOWSHEET- IS THE ANTICOAGULATION CLINIC SMARTFORM EXCEL FILE - FILE AC CLINIC USES TO TRACK THE LIST OF PATIENTS AND NUMBER OF REMINDER CALLS MADE. 14 4. Initiation of warfarin therapy: a. Obtain Baseline INR. b. Begin warfarin at 5 - 10 mg daily (may need lower dose such as 2-2.5 mg/day in patients with coexisting medical problems, concurrent interacting medications or with known or suspected sensitivity to warfarin. Have patient take warfarin in the evening. c. Return to clinic or laboratory for INR testing as specified in B.5 5. Initiation of anticoagulation therapy will require frequent INR blood tests and subsequent dosage adjustments until the patient is anticoagulated and the INR results are stable (defined as two similar, consecutive therapeutic INRs). The AC Clinic will use the consensus guidelines for the frequency of INR monitoring as follows: a. After initiation of warfarin therapy, INR drawn at least weekly until stable. b. Then every 2 weeks until stable. c. Then every 4 weeks unless special circumstances exist. d. If previously stable INR, becomes unstable then proceed back to a. or b. above. e. If INR is slightly out of range, repeat within 1 month. If still out of range then adjust warfarin regimen. 6. For inclinic appointments, vital signs (blood pressure, pulse, etc.) should be measured if not done within last 48 hours, then documented in the medical record. Patients arriving early will be seen as soon as possible. Walkins will be seen as soon as possible as space permits in the AC Clinic schedule. 7. If a patient develops uncontrolled bleeding, signs and symptoms of thromboembolism. etc., the patient will be instructed to go to the nearest Emergency Room or call 911. 8. Using the guidelines below established by the Dean Clinical Practice Committee for Anticoagulation Bridging, the AC Clinic clinician will consult with the appropriate provider to arrange a care plan for managing anticoagulation therapy perioperatively and around other invasive procedures: 15 16 Clinical Practice Committee Anticoagulation Bridging Algorithm Bridging Regimens HIGH THROMBOEMBOLIC RISK- VTE 1 4 days prior to procedure- discontinue warfarin 2 2 days prior – start Full Dose Enoxaparin (1mg/KG BID) 3 12 hours prior – discontinue Enoxaparin 4 Day of procedure – check INR, should be <1.5 5 Evening of the day of procedure – restart warfarin 6 Approximately 12 hours post procedure – restart Full Dose Enoxaparin 7 3-5 days post – begin regularly monitoring INR, stop Enoxaparin when INR > 2. NOTE: In pregnant patients continuous unfractionated heparin should be used unless anti-factor Xa activity is measured and the dose of Enoxaparin appropriately adjusted. HIGH THROMBOEMBOLIC RISK- MECHANICAL HEART VALVE(MHV) Unfractionated heparin has been the standard bridging anticoagulant for patients with mechanical heart valves. Early studies with Low Molecular Weight Heparin (LMWH) bridging revealed an increased thromboembolic risk in pregnant women with MHV’s. It is now known that LMWH doses require adjustment in pregnancy to account for altered metabolism of the drug (based on measurements of anti-Xa activity). However, because of inadequate comparative trials the American College of Cardiology/American Heart Association gives its highest recommendation (Ia) to the use of UFH as outlined below with a IIb recommendation for the LMWH regimen outlined above for VTE. 1 4 days prior to procedure - discontinue warfarin 2 2 days prior (or when INR<2.0) start continuous UFH maintaining aPTT 55-70 3 6 hours prior discontinue heparin 4 Day of procedure – check INR, should be <1.5 5 Evening of the day of procedure – restart warfarin 6 Approximately 12 hours post procedure – restart UFH, continuing until INR>2.0 INTERMEDIATE THROMBOEMBOLIC RISK This is a heterogeneous group with a relatively low, however broad range of thromboembolic risk during this brief period of inadequate anticoagulation. The vast majority of these patients do not achieve a significant clinical benefit from bridging and can thus be managed using the Low Thromboembolic Risk strategy. The Department of Cardiology at Dean does not bridge this group of patients unless they have had a recent embolic event (i.e. stroke). LOW THROMBOEMBOLIC RISK 1 2 3 4 days prior - discontinue warfarin Day of procedure – check INR, should be <1.5 Day of procedure – restart warfarin 17 C. Patient Interview and Assessment Initial assessment 1. During the initial interview the AC Clinic Clinician will: a. gather data from the medical record and information from patient including: complete medical history family history of bleeding and/or clotting disorders current medications list (including supplements and OTC drugs) social, lifestyle, and employment profile health beliefs and attitudes level of understanding health literacy personal health motivation healthcare resources b. explain anticoagulation therapy to the patient and/or caregiver c. provide a medium for alerting others that the patient is anticoagulated (i.e., Medic d. discuss operational aspects of the AC Clinic. Provide first appointment information e. obtain a reliable means of communication with the patient to be able to discuss INR results and implement a care plan (phone numbers, cell numbers, MyChart, contact numbers) f. determine the patient’s level of understanding of their disease and therapy g. assess the patient’s ability or willingness to comply with therapy and clinic visits h. assess any significant risk(s) for bleeding and falls i. assess level of alcohol use or abuse j. assess significant drug and dietary interactions k. provide education to the patient and/or caregiver or relative regarding the importance of regular monitoring of INRs, regular follow-up, drug-food and drug-drug interactions, and signs/symptoms of bleeding (see Attachment: Patient Education Record). The patient or caregiver will be given written information regarding warfarin (see Attachment: Warfarin Patient Education Guide) Follow-up and Assessment 1. All patients will be questioned using the following criteria (but not limited to): a. b. c. d. e. f. g. current anticoagulant dose signs and symptoms of bleeding recent alterations of diet, medications or alcohol intake changes in lifestyle and/or health status compliance with anticoagulation regimen status of specific medical indication requiring anticoagulant therapy status of other disease states or acute problems unrelated to anticoagulation 2. Evaluation of the patient will include an interview either face-to-face or per phone and an assessment of the patient’s laboratory results relating to anticoagulation therapy 3. When assessing for recently added medications, the AC Clinic clinician will screen for drug interactions with anticoagulation therapy. Based on the clinical significance of the potential interaction, the AC Clinic clinician may contact the physician and suggest use of alternative non-interacting medication if available 18 Alert Bracelet) D. Dosage Adjustments 1. Based on the objective and subjective findings in the patient and the Collaborative Care Agreement, the AC Clinic Clinician may adjust or make recommendations to adjust the anticoagulation regimen to keep the patient’s INR (or other lab test) in the desired range utilizing the guidelines below: Warfarin Dosage Adjustment Guidelines If the measured INR is out of the desired ranges below consider the following warfarin dosage adjustment based upon weekly dosage. If INR is only minimally out of range no dosage adjustment may be required. Measured INR < 2.0 3.0 - 3.5 3.6 - 5.0 5.1 – 9.0 (no bleeding) Goal INR 2.0 - 3.0 Weekly Warfarin Dose by 5-15% by 5-10% If needed hold 1 dose and by 5-15% Hold 1-2 doses, Check INR and resume warfarin at 10-20% when INR in range Contact MD to discuss treatment options Goal INR 2.5 - 3.5 Weekly Warfarin Dose by 5-15% No change needed If needed hold 1 dose and by 5-15% Hold 1-2 doses, Check INR and resume warfarin at 10-20% when INR in range Contact MD to discuss treatment options Comment* Alternatively: hold 1 dose, contact MD to consider vitamin 2.55mg orally x 1 dose if high risk for bleeding or if urgent surgery required. If INR still elevated after 24 hours can repeat with vitamin K 1.25-2.5mg orally x 1 dose. >9.0 (no Hold warfarin, consider vitamin 2.5-5mg orally x 1 dose. bleeding) Expect INR decrease in 24-48 hours. Can repeat vitamin K 2.55mg orally based on repeat INR values if needed. When INR in therapeutic range resume warfarin 15-20%. Serious bleeding Contact MD to discuss Contact MD to discuss Hold warfarin. Send patient immediately to ER. vitamin 10mg at any INR treatment options treatment options IV over 1 hour, FFP. Can repeat vitamin K every 12 hours elevation based on INR values. Life-threatening Contact MD to discuss Contact MD to discuss Hold warfarin. Send patient immediately to ER. FFP, bleeding treatment options treatment options supplement with viamin K 10mg IV over 1 hour. Can repeat FFP, vitamin K *Do not use the subcutaneous route for vitamin K administration. Oral administration is route of choice. Use IV only as above with telemetry and close monitoring of patient(i.e., ER, ICU, etc.). *Can expect a significant reduction in INR within 24 hours of vitamin K administration. *Contact supervising physician or physician on call if any significant problems develop. *Do NOT give Vitamin K to patients on warfarin with artificial mechanical valves per CV Surgery Department 2. Patients whose INRs have been stable, who now present with an INR outside of the desired range will be questioned in an attempt to identify the responsible factors, which, if controlled, would eliminate the need for dosage adjustment. If no reasonable factor is identified, the warfarin dose will be adjusted based upon past dosing history, kinetic parameters and dosage adjustment guidelines Return visits will be scheduled according to the established guidelines. a. If the measured INR is lower than the desired therapeutic range, the AC Clinic clinician will assess for compliance with the regimen, drug interactions, dietary alterations, excessive alcohol use, fever and overall health status. The AC Clinic clinician will increase the dose or recommend a dosage increase based on established guidelines and clinical judgement. b. If the measured INR is higher than the desired range consider adjustment in dosage per guidelines above. Carefully monitor therapy to regain control if no signs of bleeding. If the measured INR is >9.0, the AC Clinic clinican will hold the warfarin and update the primary or on-call physician regarding the patient’s condition and plan a course of action. 3. The AC Clinic will inform the patient of the INR result and of any changes in care plan. 19 When possible, patients will be given a written dosing schedule for their anticoagulation therapy which takes into account dosage adjustments, tablet strength, INR result, next appointment date and telephone number to call with questions or problems (see warfarin dose card below). Name_____________________________________ Date__________________ Tablet Size________________________ INR Result______________________ Warfarin Schedule (number of tablets to take daily): Monday ___________ Tuesday ___________ Wednesday ___________ Thursday ___________ Friday ___________ Saturday ___________ Sunday ___________ Next Appointment__________________ Blood Draw______________________ If questions or problems, call__________________________________________ 4. The AC Clinic clinician will fax a prescription to the patient’s pharmacy on behalf of primary physician for the specific anticoagulation medication in accordance with the Collaborative Care Agreement. 20 E. Patient Education 1. The educational component may be the most important aspect of successful control of anticoagulation therapy. Each patient or caregiver will be instructed during an AC Clinic office visit or via telephone according to their needs and abilities using the guide below: Dean Anticoagulation Clinics PATIENT EDUCATION GUIDE Please review the items below with patient/caregiver and document in Epic: 1. Rationale for warfarin therapy. Patient understands Indication for warfarin therapy. How warfarin works. 2. Warfarin regimen. Patient understands Dosage strength, tablet color, brand name. Planned duration of therapy. The need for compliance with regimen: Take only as prescribed. Patient to refer to dosing card or warfarin calendar. Take warfarin at the same time daily (5:00 PM if possible). Missed doses: take the same day if missed earlier that day; if it is the next day take the usual dose. Do not double the dose. Report the missed dose to the pharmacist at next clinic visit. To keep a sufficient supply of warfarin available for trips, vacations, etc. 3. INR tests. Patient understands What the INR test is, desired range, need for regular INR blood draws. Who to call if patient misses a clinic visit or scheduled blood draw. 4. Factors affecting the INR. Patient understands Diet and Vitamin K intake needs to be consistent. Avoid both binge eating and crash diets. Alcohol consumption limited to 1-2 drinks per day. Avoid excessive intake. That other medications including OTCs can influence the action of warfarin. To tell the AC Clinic clinician if changing, starting, or stopping doses of other medications. To avoid taking aspirin-containing or NSAID-containing products unless prescribed by the physician. Avoid smoking and chewing tobacco (at a minimum be consistent). 5. Warning signs. Patient understands The need to report ANY signs of bleeding to the pharmacist, nurse or doctor. What to do if any of the following occur: Skin rash. Fever or developing illness. Pain, swelling, excessive bruising, discomfort. Prolonged bleeding from cuts, nosebleeds, excessive bleeding from gums while brushing teeth, increased menstrual flow. Discoloration of the urine (pink, cherry red) and stool (black tarry, amber, red). 6. Miscellaneous patient factors. The patient understands To avoid physical activities such as sports or hobbies that may cause injury. To be careful when using sharp objects during work or at home. 21 To keep physical activity consistent. To use soft bristle toothbrush. To use an electric razor for shaving if possible. To use care when getting in/out of bathtub shower. To use care when walking outside during the winter if slippery. The need to inform other doctors, dentists or other health care providers that patient is taking warfarin. NOT to take warfarin during pregnancy. Need to discuss with doctor. 7. Patient provided with Warfarin Medication Guide Information about wearing a Medical Alert Bracelet or carrying a Coumadin user card. F. Documentation 1. The AC Clinic clinican will record all objective and subjective findings in the Anticoagulation Section of the computerized medical record (Epic). All pertinent patient anticoagulation data and patient-clinician interactions will be documented in the Anticoagulation Section of Epic, each encounter completed and signed by the AC Clinic clinician. All data must appear the the patient’s Anticogaulation Flowsheet in Epic. G. Billing (still developing) 1. Billing to Medicare and other insurance carriers for AC Clinic patients is done in the Epic encounter under Level of Service on the Visit Navigator. a. For patients managed by the AC Clinic via an inclinic appointment: i. An “incident to” or “Office Visit, Est, Level 1” charge (CPT 99211) can be billed by the AC Clinic clinician under Level of Service using the supervising physician for the AC Clinic or the on-call Internal Medicine physician for the day provided that: a. the patient must NOT have an appointment with the supervising physician, or another physician/advanced practitioner in same department, or with the on-call Internal Medicine physician on the same day as the patient’s AC Clinic appointment. b. the supervising physician, or another physician/advanced practitioner in the same department, or the oncall Internal Medicine physician of the day must be inclinic at the time of the patient’s AC Clinic appointment. c. if points a., and b., are not fully met, then the AC Clinic clinician will enter “Epic care No Charge” under Level of Service on the Visit Navigator. No charge will be billed to Medicare or other insurance carrier. ii. If the patient has an appointment with a provider who is the NOT the supervising physician, or another physician/advanced practitioner in the same department, or Internal Medicine on-call physician for the day, then then AC Clinic clinician can bill a Level 1 (CPT 99211) charge. iii. For patients whose INR test is performed by the AC Clinic clinician using a portable INR monitor: a.……………(being developed) b. For patient managed by the AC Clinic via the telephone, letter, or MyChart: i. The AC Clinic clinician will enter “Epic care No Charge” under Level of Service on the Visit Navigator. No charge will be billed to Medicare or other insurance carrier. 22 Ansell JE, Butarro ML, Thomas OV, Knowlton CH and the Anticoagulation Task Force. Consensus Guidelines for Coordinated Outpatient Oral Anticoagulation Therapy Management. Ann Pharmacother 1997;31:604-15. Hirsh J, Dalen JE, Deykin D, Poller L, Bussey H. Oral anticoagulants: mechanism of action, clinical effectiveness and optimal therapeutic range. Chest 1995;108(suppl):231S-46S. (update) 23