Ch. 4 Blood Flow and Metabolism
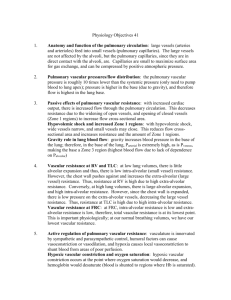
Right Ventricle Pulmonary Artery Terminal Bronchioles plexus capillaries
Pressures w/in Pulmonary BV’s
Pressures in pulmonary circulation are remarkably low
Pulmonary artery 15mm Hg (systolic – 25mmHg; diastolic –8 mmHg)
Pressure @ inlet 10 mmHg; pressure @ outlet ~100 mmHg
Pulmonary vasculature – contain very little SM o Responsible for accepting 100% of CO o Rarely concerned with directing flow – keeps Rt. Heart small
Pressures usually b/t 12 mm Hg and 8 mm Hg
Pressures around Pulmonary BV’s
Pulmonary capillaries are virtually surrounded by gas
If alveolar pressure >> capillary pressure collapse occurs
Transmural pressure (Pin – Pout) – for capillary to NOT collapse – P
TM
>> P
A o In other words—as long as transmural pressure is positive – collapse is prevented; and if transmural pressure (w/in the cap) becomes negative – collapse will occur (( d/t pressure of alveoli on the capillary))
Both pulmonary arteries and veins increase their pressure (w/in) during inspiration o Large BV’s (i.e. pulmonary artery) – “extra-alveolar vessels” – includes arteries and veins that run through the lung parenchyma
Caliber/diameter is greatly affected by lung volume b/c this determines the expanding pull of the parenchyma on their walls
Very large vessels near the hilum are outside of the lung substance and are exposed to intrapleural pressure o Small BV’s (i.e. capillaries) – “alveolar vessels”
Caliber/diameter determined by the relationship b/t alveolar pressure and pressure inside (i.e. Transmural pressure)
Summary of Alveolar and Extra-Alveolar Vessels o Alveolar vessels are exposed to alveolar pressure and are compressed if this increases
(again, if Transmural pressure 0 and then negative; collapse occurs) o Extra-alveolar vessels are exposed to a pressure less than alveolar, and are pulled open by the radial traction of the surrounding parenchyma
Pulmonary Vascular Resistance
Vascular resistance = (input pressure – output pressure) / blood flow
Pressure drop across pulmonary vasculature ~ 10 mm Hg; therefore pulmonary vascular resistance is about 1/10 th of systemic
Pulmonary blood flow = 6 L/min
Pulmonary vascular resistance = (15-5) / 6 ~= 1.7 mm Hg/(1/L)/min
Pulmonary resistance decreases as pressure increases o Why? o 1) Recruitment: under normal conditions, some cap’s are either closed, or open – but receive little or no blood flow (i.e. apex of lung) --- as pressure rises, these vessels begin to conduct blood, thus lowering the overall resistance (i.e. in parallel)
Chief mech. For the fall in pulm. Vascular resistance that occurs as the pulmonary artery pressure is raised from low levels o 2) distension: at higher capillary pressures, distension occurs (vasodilation)
Predominant mechanism for the fall in pulmonary vascular resistance at relatively high vascular pressures
Remember: a positive transmural pressure = distending pressure (i.e. how you prevent collapse of trachea on expi w/ large drop in pressure in airways)— cartilage provides the increase in transmural pressure b/t airway (pressure forcing expansion) and lungs (pressures promoting collapse) o 3) lung volume: capillaries are pulled open as the lung expands vascular resistance is low at large lung volumes
Also, the capillaries have a high resistance when lung volumes are low (i.e. max expi or at FRC, or RV)
Critical opening pressure – amt. of pressure that pulmonary artery must provide for collapsed vessel’s Pressure to be equal and opp. To pleural pressure
(i.e. restore a positive transmural(distending pressure) once a negative transmural pressure/collapse has occured
Lung Volume o EPP (equal potential pressure) or Critical opening pressure o EPP occurs where the pressure in the capillary is equal to the pressure in the alveolus o If EPP occurs within the lower airways collapse of vessel occurs o The vessel cannot be openend until the pressure of the capillary becomes equal to or greater than the pressure w/in the alveolus critical opening pressure (see animation) o Even if the pressure in the cap’s is not changed w/ large lung inflations (inspi), the capillaries resistance increases o Drugs that cause contraction of pulmonary vessels (i.e. Beta 2 agonist—albuterol, ach, isoproterenol) cause contraction of the SM increasing pulmonary vascular resistance
(i.e. increasing flow)
Serotonin, histamine, norepi—potent vasoconstrictors
Prostacyclin – potent vasodilator o Summary of Pulmonary Vascular Resistance
It is normally very small
Decreases on exercise b/c of recruitment and distention of capillaries
Increases at high and low lung volumes
Increases with alveolar hypoxia b/c of constriction of small pulmonary arteries
Measurement of Pulmonary Blood Flow
Fick principle: o The O2 consumption per minute (dot VO2) is equal to the amt. of O2 taken up by the blood in the lungs per minute o B/c the O2 concentration in the blood entering the lungs is C(line)VO2 and blood leaving is CaO2 :
(dot)Q ((Perfusion)) = Ventilation of O2 / (Concentration of arterial O2 –
Concentration of blood entering the lungs)
Q = V
O2
/ (C aO2
– C
VO2
)
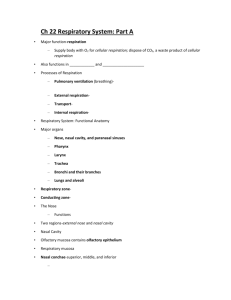
Distribution of blood Flow
Blood flow decreases linearly from bottom to top, reaching very low perfusion values at the apex
Distribution of blood is dependent on posture and exercise
Supine position: apical zone blood flow increases, but the basal zone flow remains unchanged
Uneven blood flow is d/t hydrostatic pressure differences w/in bv’s. o Zone 1 aka Alveolar Dead Space
P
A
> P a
> P
V
– where pulmonary arterial pressure falls below alveolar pressure – capillary collapse (negative P
TM
)
normally doesn’t occur b/c the pulmonary arterial pressure is sufficient to raise blood to top of the lung but may occur if arterial pressure drops (i.e.
hemorrhage) or if alveolar pressure is raised (i.e. positive ventilation) o Zone 2
P a
> P
A
> P v
Pulmonary arterial pressure >> alveolar pressure
Venous pressure << alveolar pressure
Blood flow is determined by the difference b/t arterial and alveolar pressures o Zone 3
P a
> P
V
> P
A
Venous pressure exceeds alveolar pressure
Transmural pressure is positive throughout length of tube
Mean width increases
Recruitment can increase blood flow in this zone o Zone 4
Region of reduced blood flow, occurs when lung is poorly inflated
At low lung volumes, the resistance of extra-alveolar vessels becomes important, and a reduction of regional blood flow is seen starting at base
General Blood Flow: Periphery << Central regions
Active Control of Circulation
Importance: o Effect of directing blood flow away from hypoxic regions of the lung ( i.e. d/t obstruction) o Assist in matching V/Q ratio (i.e. ventilation to perfusion = 1/1 normally) o Occurs at high altitude
Hypoxic pulmonary Vasoconstriction – P
A
O2 is reduced
Occurs when PAO2 << 70 mm Hg (normal PA/aO2 = 100 mm Hg) o Contraction of SM in the walls of the small arterioles in the hypoxic region o Not dependent on CNS connections o Vasoconstriction is determined by: PA
O2
Decreased PAO2 Inhibition of voltage gated K+ channels Increased cytoplasmic Ca++ SM contraction Increased pulmonary vascular
resistance o Fetal
Relatively low oxygen
High pulmonary resistance
First Breath removes hypoxic vasoconstriction
Increased O2
Decreased pulmonary vascular resistance o NO mech.
Block NO increase Hypoxic Vasoconstriction
Adm. NO reduce hypoxic vasoconstriction (20mm usually, lethal at high doses)
NO is created from L-arginine via catalysis by eNOS
NO activates cyclic GMP SM relaxation
o Pulmonary endothelial vasoconstrictors
Endothelin-1 (ET-1)
Thromboxane A
2
(TXA
2
)
o Other causes of vasoconstriction:
Decreased pH (i.e. anaerobic metab.)
Increased sympathetic activity
Hypoxic Pulmonary Vasoconstriction o Alveolar hypoxia constricts small pulmonary arteries o Probably a direct effect of the low PaO2 on vascular smooth muscle o Critical at birth in the transition from placental to air breathing o Directs blood flow away from poorly ventilated areas of the diseased lung in the adult o PAO2 of 100 mm Hg = 80 % flow (normal) o PAO2 of 50 mm Hg = 40% flow (vasoconstriction) o PAO2 of 150 mm Hg = 90% flow (i.e. adm NO)
Water Balance in the Lung
Distance b/t capillary blood from alveolar air = 0.3 µm
Fluid exchange across capillary endothelium obeys Starling’s law o Force tending to push fluid out of the capillary is hydrostatic pressure minus the hydrostatic pressure of the interstitial fluid ( P
C
– P i
) o Force tending to pull fluid in is the osmotic pressure of the proteins of the blood minus that of the proteins of the interstitial fluid (π
C
– π i
) o σ – is the effectiveness of the capillary wall in preventing the passage of proteins across it; termed reflection coefficient o K = filtration coefficient o Net fluid out = K[(P
C
– P i
) – σ (π
C
– π i
) o Capillary osmotic pressure ~ 28 mm Hg o Colloid osmotic pressure of interstitial fluid ~ 20 mm Hg o Net result: outward Pressure – causes about 20ml/hr to diffuse from capillary into interstitium
Where does the fluid go? o Fluid which leaks out into the interstitium of the alveolar wall tracks through the interstitial space to the perivascular and peribronchial space w/in the lung
Numerous lymphatics brings this fluid to hilar lymph nodes o Interstitial edema -- Earliest form of pulmonary edema is characterized by engorgement of the peribronchial and perivascular spaces o Later stage of pulmonary edema – fluid may cross the alveolar epithelium into the alveolar spaces
Alveoli fill w/ fluid one by one, and b/c they are unventilated no diffusion occurs (i.e. no oxygenation & no removal of CO2) o Fluid that reaches the alveolar spaces is actively pumped out by Na+,K+, and ATPase pumps in epithelial cells o Seriousness: alveolar edema >>>> interstitial edema
Other Functions of the Pulmonary Circulation (see Ch.1 summary)
Acts as reservoir of blood
Ability to reduce pulmonary vascular resistance as its vascular pressures are raised through: recruitment and distension o Same mechanism allows lung to increase its blood volume w/ relatively small rises in pulmonary arterial or venous pressures. (i.e. change in posture from standing supine)
Blood then drains from legs lung
Acts as a filter for blood o Small thrombi are removed from the circulation before they can reach the brain or other vital organs o Traps WBC’s (fx unknown)
Metabolic Functions of the Lung
See chart Ch.1 summary
Activated in lung: o Vasoconstrictors:
Angiotensin I angiotensin II
Angiotensin II has NO effect on the lung vasculature itself (i.e. effects systemic vasculature)
ACE located in small pits on surface of capillary endothelial cells
Inactivated in lung: o ACE o Vasodilators:
Bradykinin (80% inactivated) o Uptake and storage of serotonin (almost completely removed) o PGE1, PGE2, PGF2α o NE o Histamine
Arachadonic acid and Metabolites released in blood o Membrane-bound phospholipid o ↓ ←Phospholipase A2 o Arachidonic Acid o Lipoxygenase→↙ ↘←Cyclooxygenase o Leukotrienes Prostaglandins, thromboxane A2
Prostaglandins are potent vasodilators and vasoconstrictors o PGE2 – relaxes patent ductus arteriosus o Also effects kallikrein-kinin clotting cascade o Asthma?
Misc: o Mast cells containing heparin in interstitium
o IgA – antibiotic defense o Synthesis of surfactant by type II pneumocytes o Leukocytes cause of emphysema via breakdown of elastin and fibrin? o Carbohydrate metabolism (via mucopolysaccharides in mucus)
 0
0