O32 DEVELOPMENT OF DISTAL TUBULAR DYSFUNCTION

O32
DEVELOPMENT OF DISTAL TUBULAR DYSFUNCTION ASSOCIATED WITH MUTATIONS IN HNF1B
Dr Shazia Adalat Dr Detlef Bockenhauer Professor Robert Kleta Professor Adrian Woolf
Great Ormond Street Hospital
Problem: We previously described urinary magnesium (Mg) wasting in a cohort of children with HNF1B mutations due to altered transcription of FXYD2, the gamma-subunit of the Na+ K+ ATPase. As this baso-lateral pump has importance beyond magnesium transport, further disturbances of electrolyte transport in the distal convoluted tubule (DCT) would be expected.
Purpose: We sought to define tubular transport abnormalities in DCT in patients with HNF1B mutations. We also aimed to elucidate the clinical course of the tubular dysfunction.
Design: Retrospective analysis was undertaken of biochemical parameters in a cohort of patients with renal tract malformations with known HNF1B mutation status. Data from HNF1B mutation carriers (mut+) was compared with that of
HNF1B mutation negative patients (mut-). Biochemical data was extracted from the pathology results database of the hospital for all available specified results: these included for plasma measurements: creatinine, Mg, chloride (Cl), potassium (K), and sodium (Na). Urinary parameters included, calcium (Ca) and Mg and creatinine to calculate their respective fractional excretion. Only those laboratory results were included, which reflected native kidney function. Height data to estimate GFR was taken from patients’ clinical notes. Median values for each biochemical parameter for each patient were calculated for each year of age with available data. Analysis of differences between mutation carriers and those without mutations was performed using non-parametric tests. Findings: The mut+ (N=31) and mut- (N=42) groups were comparable with respect to age at first available data set (median 2 years (range 0.9-15.8 years) vs. 1.4 years
(range 0.9-13.8 years) ; p=0.18), estimated GFR at this time (median 65 (range11-144) ml/min/1.73m2 vs. 59.4 (range 8-
109); p=0.56); and age at last available dataset (median 11.9 years (range 1.6-17.8 years) vs. 11.59 years (range 3.3-
18.5 years); p=0.68) and GFR at that time (median 63.4 (range 4.9-135) vs. 74 (range 6-141) ml/min/1.73m2 ;p=0.26).
Statistically significant differences were found for median plasma Mg, K and Cl measurements (all p<0.001) between the 2 groups but not for plasma Na.
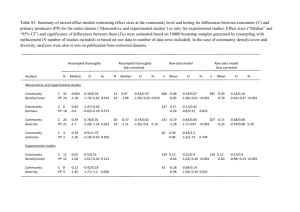
Median magnesium measurements in HNF1B mut+ (shaded boxes) and mut- (unshaded boxes) patients p=0.0037
p=0.453
p=0.278
1.75
1.50
1.25
1.00
0.75
0.50
p<0.001
p<0.0001
p=0.0014
0.25
1 Age <1 1 5 Age 5 5 10 15
Year of life
Median plasma Mg levels were not significantly different between the two groups in the first year of life. There was a significant fall in Mg in mut+ patient between the 1 st and 5 th year of life (p<0.05). Median Mg measurements were significantly different between groups from the age of 5 years (p<0.001). Fractional excretion of Mg calculations where available (n=15) confirmed that all mut+ patients tested had inappropriately high fractional excretion of urinary Mg (all
>4%). Hypocalciuria was present in 14 mut+ patients where data was available on urinary Ca excretion. Fractional excretion of Ca was calculated to be below 0.5% in all of these patients and remained below this up to the point of last follow-up.
Similar to plasma Mg, there was a decline in median plasma Cl and K levels in mut+ patients, with a significant difference between both groups present at 10 years of age (p<0.01) between the two groups. There was no statistical difference in
Na measurements at any age.
Conclusion: We provide evidence for a generalised disturbance in DCT transport. Interestingly, the tubular dysfunction evolves over time, suggesting a developmental change in DCT function over the first years of life. Relevance:
Hypomagnesaemia in patients with renal malformations is often used as an indication to perform HNF1B analysis. Our data indicate that biochemical abnormalities during early childhood are an unreliable indicator for HNF1B testing.
Moreover, our data provides novel information on the development of DCT transport.