Imaging Service Request Form (Opens in a new window)
advertisement
")
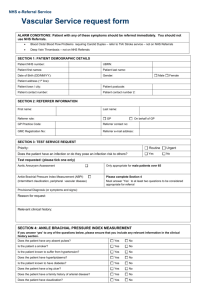
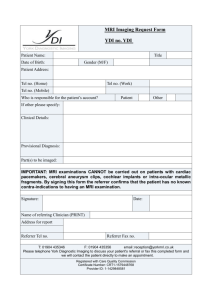
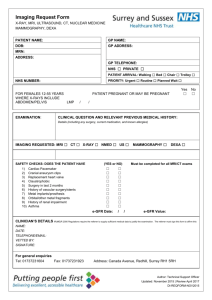
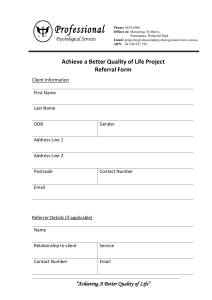
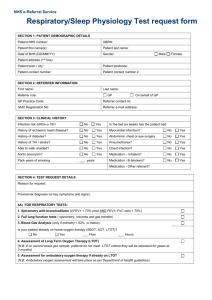
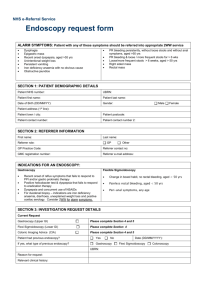
NHS e-Referral Service Imaging Service request form SECTION 1: PATIENT DEMOGRAPHIC DETAILS Patient NHS number: UBRN: Patient first names: Patient last name: Date of Birth (DD/MM/YY): Gender: Male st Patient address (1 line): Patient town / city: Patient postcode: Patient contact number: Patient contact number 2: SECTION 2: REFERRER INFORMATION Referrer first name: Referrer last name: Referrer role: GP Other, Please specify: GP Practice Code: Referrer contact no: GMC Registration No: Referrer e-mail address: SECTION 3: IMAGING SERVICE REQUEST Imaging procedure requested (include left / right where relevant) Referral date: Priority: Routine Urgent Provisional diagnosis (or key symptoms and signs): Clinical question to be answered, relevant clinical history and previous imaging: (if available attach imaging results) N.B. The referrer must provide sufficient clinical information to justify the request. SECTION 4: CLINICAL SAFETY QUESTIONS If you answer ‘Yes’ to any of the questions, please ensure that you include any relevant clinical information above. Does the patient present a communicable infection risk? No Yes Is the patient known to be pregnant? No Yes Has the patient had a previous allergic reaction to contrast? No Yes Is the patient known to have renal impairment? No Yes Is the patient at risk from cardiac failure? No Yes Is the patient on Metformin ? No Yes Does the patient have asthma? No Yes Does the patient have any implanted metallic foreign devices? (e.g. cardiac pacemaker, artificial heart valve, cerebral aneurysm clips, cochlear implant, etc.) No Yes Is the patient known to have metallic fragments in their eyes? No Yes Is the patient known to suffer from severe claustrophobia? No Yes Is the patient known to have renal impairment? No Yes COMPLETE FOR ALL CT AND IVU REQUESTS COMPLETE FOR ALL MRI REQUESTS COMPLETE FOR ALL OBSTETRIC ULTRASOUND REQUESTS Parity: Gravida: Date of LMP or number of weeks pregnant: Female