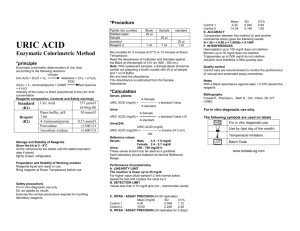
Serum uric acid level.
advertisement

G- 02: nutrition F-08: cardiovascular complications Relationship Between Serum Uric Acid and All-Cause and Cardiovascular Mortality in Patients Treated With Peritoneal Dialysis Xi Xia, MD∗ ,Feng He, MD∗,Xianfeng Wu, MD, Fenfen Peng, MD ,Fengxian Huang, MD, PhD ,Xueqing Yu, MD, PhD American Journal of Kidney Diseases Volume 64, Issue 2, Pages 257–264, August 2014 Department of Nephrology, The First Affiliated Hospital, Sun Yat-Sen University, Guangzhou, China ABSTRACT Although serum uric acid level appears to be associated with mortality in individuals treated with hemodialysis, the relationship between serum uric acid level and death is uncertain in patients treated with peritoneal dialysis (PD). Study Design Cohort study. Setting & Participants 985 patients from a single PD center in South China followed up for a median of 25.3 months. Predictor Serum uric acid level. Outcomes & Measurements The association of baseline sex-specific uric acid level with all-cause and cardiovascular mortality was evaluated. Models were adjusted for age, body mass index, comorbidity score, residual kidney function, total Kt/V, allopurinol and angiotensin-converting enzyme inhibitor/angiotensin receptor blocker use, and laboratory test results, including hemoglobin, serum albumin, creatinine, calcium, phosphorus, triglycerides, low-density lipoprotein cholesterol, and high-sensitivity C-reactive protein. Results Mean age was 48.3 ± 15.4 (SD) years, and 23% had diabetes. Mean uric acid level was 7.0 ± 1.3 (range, 3.8-19.8) mg/dL. During follow-up, 144 deaths were recorded, of which 64 were due to cardiovascular events. In multivariable models, the highest sex-specific tertile of uric acid level was associated with increased risk of all-cause mortality (HR, 1.93; 95% CI, 1.272.93; P = 0.004) and cardiovascular mortality (HR, 3.31; 95% CI, 1.70-6.41; P < 0.001) compared to the lowest tertile. Adjusted Cox regression models showed that the HRs per 1mg/dL higher uric acid level for all-cause and cardiovascular mortality were 1.33 (95% CI, 1.14-1.56; P < 0.001) and 1.44 (95% CI, 1.17-1.77; P = 0.001) for men and 1.03 (95% CI, 0.86-1.24; P = 0.8) and 1.16 (95% CI, 0.97-1.38; P = 0.1) for women, respectively. A formal test for interaction indicated that the association of uric acid level with all-cause and cardiovascular mortality differed by sex (β = −0.06 [P = 0.02] and β = −0.10 [P = 0.02], respectively). Limitations Single measurement of uric acid at baseline. Cause of death determined by death certificates and expert consensus. Conclusions Elevated serum uric acid level is an independent risk factor for all-cause and cardiovascular mortality in men treated with PD. Index Words: Serum uric acid, peritoneal dialysis, all-cause mortality, cardiovascular mortality COMMENTS Uric acid is the final product of purine nucleotide metabolism in humans. 4 Increased serum uric acid levels have been shown to be related to kidney disease, CVD, hypertension, and metabolic syndrome. The large multicenter international study (DOPPS [Dialysis Outcomes & Practice Patterns Study]) found that higher uric acid levels were associated with a lower risk of all-cause and CV mortality in the hemodialysis population1 The studie mainly focused on hemodialysis settings; however, the relationship of serum uric acid level and mortality is uncertain in patients treated with PD. In addition, sex-related differences in serum uric acid level– mortality have been reported, and some studies have shown serum uric acid level to be a predictor of mortality in women only. It is unclear whether uric acid level is an independent risk factor for increased all-cause and CV mortality in both male and female patients treated with PD From January 1, 2006, to November 30, 2010, a total of 985 consecutive patients were recruited from a single PD center of the First Affiliated Hospital of Sun Yat-sen University. Enrollment included all patients aged 18-80 years who had received continuous ambulatory PD for more than 3 months, except those who had malignant disease or refused to give written consent. CVD was defined as history of angina pectoris, myocardial infarction, angioplasty, coronary artery bypass, heart failure, or stroke. The Davies score assigns 1 point for each of the following conditions: ischemic heart disease (defined as prior myocardial infarction, angina, or ischemic changes on electrocardiogram), left ventricular dysfunction (defined as clinical evidence of pulmonary edema not due to errors in fluid balance, or history of congestive heart failure), peripheral vascular disease (includes distal aortic, lower extremity, and cerebrovascular disease), malignancy, diabetes, collagen vascular disease, and other significant pathology (eg, chronic obstructive pulmonary disease).24 The theoretical range is 0-7. Each score was categorized into 4 levels: 0, 1, 2, and >2. The primary outcome of interest was all-cause mortality, and the second outcome of interest was CV mortality. CV events contributing to CV mortality included acute myocardial infarction, atherosclerotic heart disease, cardiomyopathy, cardiac arrhythmia, cardiac arrest, congestive heart failure, cerebrovascular accident (including intracranial hemorrhage), ischemic brain damage, anoxic encephalopathy, and peripheral vascular disease. Participants were stratified into tertiles of serum uric acid levels, which were calculated separately in men (tertile 1 [lowest], <6.67; tertile 2 [middle], 6.67-7.56; and tertile 3 [highest], >7.56 mg/dL) and women (tertile 1, <6.19; tertile 2, 6.19-7.13; and tertile 3, >7.13 mg/dL, respectively). A total of 985 patients were enrolled in this study (mean age, 48.3 ± 15.4 [SD] years; 58% men; 23% with diabetes), with a median follow-up of 25.3 (maximum, 71.8) months. Mean serum uric acid value was 7.0 (range, 3.8-19.8) mg/dL for all patients, and male patients had a significantly higher mean serum uric acid level than female patients (7.2 ± 1.2 vs 6.8 ± 1.4 mg/dL, respectively; P < 0.001). With each 1-mg/dL increase in serum uric acid level, adjusted HRs of all-cause and CV mortality were 1.33 (95% CI, 1.14-1.56; P < 0.001) and 1.44 (95% CI, 1.17-1.77; P = 0.001) for men and 1.03 (95% CI, 0.86-1.24; P = 0.8) and 1.16 (95% CI, 0.97-1.38; P = 0.1) for women, respectively. As further support of this apparent difference by sex, they tested the interaction between sex and serum uric acid level on all-cause and CV mortality among all participants and observed a significant interaction (β = −0.06; [P = 0.02] and β = −0.10 [P = 0.02], respectively). So, higher serum uric acid concentrations are associated with higher all-cause and CV mortality only in male patients treated with PD. The association remained robust despite adjustment for metabolic and CV risk factors. Further studies will be necessary not only to determine whether uric acid–lowering regimens improve survival in patients treated with PD. Pr. Jacques CHANARD Professor of Nephrology