dempsey_whitakerabstract
advertisement

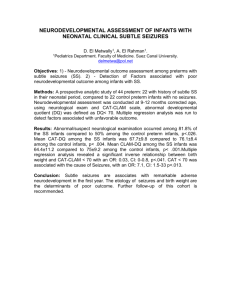
Improved Assessment of Resting State Functional Connectivity and Seizure Activity in Infants Using DOI and EEG Laura Dempsey1, Chuen Wai Lee, Rob Cooper, Harsimrat Singh, Andrea Edwards, Topun Austin2 In the UK alone over 1,000 infants born at term experience seizures, typically due to hypoxic-ischemic encephalopathy (HIE) brain injury. Infant seizures are often linked to poor neurodevelopment and can be precursors of serious neurological disorders. Electroencephalography (EEG) is the standard modality used to identify and monitor seizures at cot-side; although temporally superior, it is limited in spatial resolution. My project aims to combine the infant EEG system with diffuse optical imaging (DOI), thereby improving cot-side monitoring of brain function. DOI is non-invasive and can produce both topo- and tomographic images of regional cerebral blood flow. Combining hemodynamic DOI measurements with electrical information from EEG makes it possible to investigate cortical neurovascular coupling in a variety of circumstances, including during seizures. En route to increasing neonatal seizure detection ability, my lab also aims to study resting state functional connectivity (RSFC) globally in cortex and functional activation in sensory cortex using combined EEG and DOI in sleeping infants. Functional imaging has the capability to quantify the health of cortical networks in infants that anatomical imaging systems, such as MRI, might overlook. The ability to elucidate healthy and pathological cortical activity with our system could help Neonatologists better estimate future cognitive and motor deficits in premature and term-born infants. To accomplish these goals we have developed a soft, flexible cap that holds 13 EEG electrodes and 32 DOI fibers. After assembling all the necessary parts of the dual imaging system and obtaining ethics approval, we are currently in the process of scanning healthy control subjects (GA 37-40 weeks). Once the efficacy of the imaging system can be verified, we will move on to scanning specific age groups, ranging from extreme premature infants (GA 23-28 weeks) to late premature infants (GA 34-37 weeks), as well as infants at-risk for seizures. 1 MPhil Candidate, University of Cambridge, Churchill College, Cambridge CB3 0DS, United Kingdom, Tel: +447717264999, Email: ld419@cam.ac.uk 2 Consultant Neonatologist, Neonatal Intensive Care Unit, Box 402, Cambridge University Hospitals NHS Foundation Trust, Hills Road, Cambridge, CB2 0QQ, United Kingdom, +441223217677, Email: topun.austin@addenbrookes.nhs.uk