5007 Summerville Rd Phenix City, AL. 36867 Phone: 334-408
advertisement

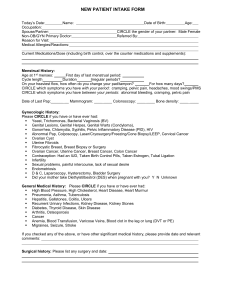
5007 Summerville Rd ● Phenix City, AL. 36867 Phone: 334-408-2854 ● Fax: 334-384-9274 www.2bridgeway.com Mammography Department Worksheet PATIENT NAME: ________________________ DATE: _______________ DOB: ________________________ Accession #: _______________ Home Phone: ________________________ Account #: _______________ Work Phone: ________________________ Ref Phys: _______________ 1. Was your last mammogram performed at Bridgeway Diagnostics (circle) yes If you answered no, list prior facility or city where you had your exam at: _____________________________________________ How old were you when you gave birth to your first child? _____________ Is there any possibility you are pregnant now? (circle) yes no Do you still have a menstrual cycle? (circle) yes no Have you had a hysterectomy? (circle) yes no Have you gone through menopause? (circle) yes no Are you currently taking hormones or steroids? (circle) yes no Do you have a family history of Breast Cancer? (circle) yes no 2. 3. 4. 5. 6. 7. 8. If yes, please indicate whom: 9. 10. no _____mother ____sister(s) ____aunt(s) ____grandmother(s) ____cousin(s) Previous Cancer? What kind? _______________________ When: _____________ Have you had any surgeries on your breast(s)? (circle) yes no If you answered yes on question number 8, which breast(s) (circle) Left Right Both Also, indicate what type of Breast surgery you had and what year you had the surgery: (Check the appropriate area) ____ Breast Implants Year ____ ____ Biopsy Year ____ ____ Lumpectomy Year ____ ____ Mastectomy Year ____ ____ Reduction Year _____ Are you having any New or Current Problems with your breast(s) today? (circle) yes no If you answered yes, please describe: 11. _____________________________________________________________ _____________________________________________________________ PLEASE RETURN THIS SHEET TO THE FRONT DESK AND YOU WILL BE CALLED BY THE TECHNOLOGIST SHORTLY. ___________________________________________________________________________ O LUMP X BIOPSY SCAR □ PAIN TECHNOLOGIST'S NOTES: __________________________________________________________ MOLE ____________________________________________________________________________________________________________________________ TECHNOLOGIST: _______________________________________