Assessment Entry Module (AEM) HEALTH SERVICE PROVIDER
advertisement
 HEALTH SERVICE PROVIDER")
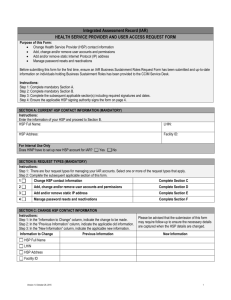
Assessment Entry Module (AEM) HEALTH SERVICE PROVIDER AND USER ACCESS REQUEST FORM Purpose of this Form: Change Health Service Provider (HSP) contact information Add, change and/or remove user accounts and permissions Add and/or remove static Internet Protocol (IP) address Manage password resets and reactivations Before submitting this form for the first time, ensure an AEM Business Sustainment Roles Request Form has been submitted and up-todate information on individuals holding Business Sustainment Roles has been provided to the CCIM Service Desk. Instructions: Step 1: Complete mandatory Section A. Step 2: Complete mandatory Section B. Step 3: Complete the subsequent applicable section(s) including required signatures and dates. Step 4: Ensure the applicable HSP signing authority signs the form on page 4. SECTION A: CURRENT HSP CONTACT INFORMATION (MANDATORY) Instructions: Enter the information of your HSP and proceed to Section B. HSP Full Name: LHIN: HSP Address: Facility ID: Assessment Type: The contacts and details on this form pertain to the following assessment types for this HSP. Please identity assessment type(s) below: Core OCAN interRAI Preliminary Screener interRAI CHA For Internal Use Only Is AEM HSP submitting assessments to the IAR? Yes No Does ESP have to set up new HSP account for AEM? (Applicable only if uploading to IAR) Yes No HINP: TransForm SSO WOHS HSN SECTION B: REQUEST TYPES (MANDATORY) Instructions: Step 1: There are four request types for managing your AEM accounts. Select one or more of the request types that apply. Step 2: Complete the subsequent applicable section of this form. 1 Change HSP contact information Complete Section C 2 Add, change and/or remove user accounts and permissions Complete Section D 3 Add and/or remove static IP address Complete Section E 4 Manage password resets and reactivations Complete Section F SECTION C: CHANGE HSP CONTACT INFORMATION Instructions: Step 1: In the “Information to Change” column, indicate the change to be made. Step 2: In the “Previous Information” column, indicate the applicable old information. Step 3: In the “New Information” column, indicate the applicable new information. Information to Change Previous Information Please be advised that the submission of this form may require follow-up to ensure the necessary details are captured when the HSP details are changed. New Information HSP Full Name LHIN HSP Address Facility ID Version 1.0 October 26, 2015 1 SECTION D: ADD, CHANGE AND/OR REMOVE USER ACCOUNTS AND/OR PERMISSIONS AEM Permissions: Data Entry – intended for non-clinical person(s) whose role is to enter assessments (from paper) into the AEM for their organization. Assessor – intended for case workers and other personnel who conduct assessments of clients of organization. Supervisor – intended for supervisory level positions that manage case workers. Supervisors can also conduct assessments for clients of their organization. Privacy – intended for the organization’s Privacy Officer. Instructions: Step 1: In the “Request Type” column, select one or more request types that apply Step 2: Enter the individual’s information in the appropriate remaining columns based on the request type Note – Additional Lines: You may insert additional lines for additional users. Request Type User Name Add New User and Permissions Version 1.0 October 26, 2015 User Email Address User Telephone AEM Permissions Data Entry Assessor Supervisor Privacy Data Entry Assessor Supervisor Privacy Data Entry Assessor Supervisor Privacy Data Entry Assessor Supervisor Privacy Data Entry Assessor Supervisor Privacy Data Entry Assessor Supervisor Privacy Data Entry Assessor Supervisor Privacy 2 Request Type Contact Information Type Current Information New Information Name User ID Change User Information and/or Permissions Not Applicable Email Address Telephone Permissions Request Type Data Entry Assessor Supervisor Privacy User Name Data Entry Assessor Supervisor Privacy User Email User Telephone User ID Remove User SECTION E: ADD AND/OR REMOVE STATIC IP ADDRESS A static external IP address is required for an HSP to access AEM . Please ensure your static IP address is an external static IP address. If you are unsure whether a static IP address is internal or external, check to see if it falls within one of the ranges listed below. If the static IP address falls within one of these numerical ranges, it is an internal IP address and cannot be used to access AEM. 10.0.0.0 – 10.255.255.255 172.16.0.0 – 172.32.255.255 192.168.0.0 – 192.168.255.255 Instructions: Step 1: In the “Request Type” column, indicate the type of request that applies. Step 2: In the “IP Address” column, list the IP addresses being added or removed as applicable. Request Type IP Address (Multiple IP addresses may be specified; please separate with a semicolon) Static IP: Add New Static IP Address Remove Static IP Address Version 1.0 October 26, 2015 3 SECTION F: MANAGE PASSWORD RESETS AND REACTIVATIONS Instructions: Step 1: Select a separate row for each user request and indicate the request type in the “Request Type” column. Step 2: Enter the individual’s information in the remaining columns as appropriate. Note – Additional Lines: You may insert additional lines for additional users Notes: Users can set up secret questions in AEM to support future password recovery. This allows users to reset their passwords electronically without having to send in a reset request. Passwords will expire after 90 days and must be reset at that time and account must be reactivated. Request Type User Name User Email User Telephone User ID Reset User Password OR Reactivate User Account Reset User Password OR Reactivate User Account Reset User Password OR Reactivate User Account Reset User Password OR Reactivate User Account Reset User Password OR Reactivate User Account HSP SIGNATURES REQUIRED HSP User Authority must sign to authorize the change. User Authority Name User Authority Email User Authority Telephone User Authority Signature Date Please complete this form in Microsoft Word have it signed and submit this form electronically to cmhcap@ccim.on.ca or csscap@ccim.on.ca Version 1.0 October 26, 2015 4