Sample Accident Investigation
advertisement

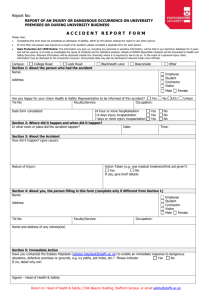
Incident & Accident Investigation Report The following incident and accident investigation report form should be completed for all associate involved accidents. The Supervisor should interview involved associates and other parties to gather the information required for this report and then complete the report. ASSOCIATE or PERSON INVOLVED IN INCIDENT INFORMATION ________________________________________________ _________________________ Employee Name _________________________________________________ Employee # ________________________________________________ Job Title _________________________ Street Address City ________________________________________________ ______ ____________ State Zip Code _________________________ Telephone Number _____________________________________________________________________________ Date of Accident Department Incident Information Specify location of incident/injury. (Where exactly did the injury happen?) ________________________________________________________________________________________________________ ________________________________________________________________________________________________________ ________________________________________________________________________________________________________ ________________________________________________________________________ Body Part Injured Injury Type Injury Cause Group Causal Factors Abdomen Abrasion Cardio Vascular Incident Body Fluid (s) Ankle Allergic Reaction Carpal Tunnel Syndrome Chemical Chest (including ribs) Bite Caught In, Under or Between Equipment Disc Bruise or Contusion Chemical Poisoning Falling Object Elbow Burn Dermatitis Lancet Eye (s) Carpal Tunnel Electrical Contact Lift/Tilt Device Finger (s) Contagious Disease Falls from Elevation Litter/Debris Foot Cumulative Trauma (all Falls on Same Level Liquid on Floor Hand Hand Tools Mechanical Failure Hip Cut or Laceration Highway Vehicles Needle Internal Organs Dermatitis (skin irritation) Machine Injuries Repositioning—Chair Knee Electric Shock Material Handling—Manual Repositioning—Bed Lower Arm Fracture or Dislocation Material Handling—Mechanical Repositioning—Bath Lower Back Area Foreign Body Misc—Not otherwise Classified Stairs, Steps Lower Leg Hernia Multiple Complaints Stool Mouth Irritation (mucus membrane) Needle Sticks/Needle Punctures Transfer—Patients Multiple Body Parts Multiple Injuries Occupational Disease—NOC Transfer—Objects Nose Sprain (Joint) Patient Handling—NOC Vehicle Sacrum and Coccyx Strain (Muscle) Slip or Trip (without Fall) Other: Shoulder (s) Other: Struck By or Against Object _____________________ Skull Struck By or Against—Other _ Soft Tissue Thumb Toe (s) Brentwood Services Loss Control other) ___________________ Person Other: _______________________ Upper Back Area (Thoracic) Wrist Multiple Parts Including Back Other: _ _____________________ _ Symptoms developed gradually over a period of time? Yes No From __________________ (date) to __________________ (date) Accident Investigation Report to be forwarded within 48 hrs. to the Corporate Health Worker’s Comp Nurse Loss Time Medical Treatment/ER Multiple Associates Involved A. Time of Injury _____ am _____ pm Time shift started __________ Damage to Hospital Property Fatality B. Phase of associate’s workday at time of injury _____ During Rest Period _____ Entering or Leaving Work _____ During Meal Period _____ Performing Work Duties _____ Working Overtime _____ Other 1. Task and Activity at time of accident General type of task ______________________________________________________________________________________________________ Specific activity __________________________________________________________________________________________________________ Employee was working _____ Alone _____ With Crew or Fellow Worker _____ Other, Specify 2. Describe how the accident occurred ______________________________________________________________________________________________________________________________ ______________________________________________________________________________________________________________________________ ______________________________________________________________________________________________________________________________ ______________________________________________________________________________________________________________________________ _________________________________________________________________________________________________________________________ 3. Root Causes. Events and conditions that contributed to the accident ______________________________________________________________________________________________________________________________ ______________________________________________________________________________________________________________________________ ______________________________________________________________________________________________________________________________ ______________________________________________________________________________________________________________________________ _________________________________________________________________________________________________________________________ 4. Corrective Action Plan. Those that have been, or will be, taken to prevent recurrence Brentwood Services Loss Control ______________________________________________________________________________________________________________________________ ______________________________________________________________________________________________________________________________ ______________________________________________________________________________________________________________________________ ______________________________________________________________________________________________________________________________ _________________________________________________________________________________________________________________________ 5. Measure of Effectiveness ______________________________________________________________________________________________________________________________ ______________________________________________________________________________________________________________________________ ______________________________________________________________________________________________________________________________ ______________________________________________________________________________________________________________________________ _________________________________________________________________________________________________________________________ Prepared by: ______________________________________ ________________________________________________ _____/_____/_____ Title: ______________________________________________ Manager/Director Signature Date Department: _______________________________________ Date: ______________________________________________ I have read the above and I agree with the description of this report. ___________________________________________________________________________ Associate’s Signature _______________________________________________ Date Injured Associate’s Comments: _________________________________________________________________________________________________ ________________________________________________________________________________________________________ ________________________________________________________________________________________________________ ________________________________________________________________________________________________________ ________________________________________________________________________________________________________ ________________________________________________________________________________________________ ACCIDENT INVESTIGATION—WITNESS STATEMENT Department: _______________________________________________________________________________________________________________ Employees Injured/Involved: ______________________________________________________________________________________________ Accident Location: _______________________________________________________________________________________________________ Accident Date: ______________________ Time: _______________ Statement Date: ___________________ Witness Name: ____________________________________________________________ Time: ________________ Telephone Number: ___________________________ Witness Address: ________________________________________________________________________________________________________ To the Witness—Briefly explain in your own words the accident. Your comments are important to help determine the Brentwood Services Loss Control causes of the accident and correct any unsafe conditions. Thank you. _______________________________________________________________________________________________________________________ _______________________________________________________________________________________________________________________ _______________________________________________________________________________________________________________________ _______________________________________________________________________________________________________________________ _______________________________________________________________________________________________________________________ _______________________________________________________________________________________________________________________ _______________________________________________________________________________________________________________________ _______________________________________________________________________________________________________________________ _______________________________________________________________________________________________________________________ _______________________________________________________________________________________________________________________ _______________________________________________________________________________________________________________________ _______________________________________________________________________________________________________________________ _______________________________________________________________________________________________________________________ _______________________________________________________________________________________________________________________ _______________________________________________________________________________________________________________________ _______________________________________________________________________________________________________________________ _______________________________________________________________________________________________________________________ _______________________________________________________________________________________________________________________ _______________________________________________________________________________________________________________________ _______________________________________________________________________________________________________________________ _______________________________________________________________________________________________________________________ _______________________________________________________________________________________________________________________ _______________________________________________________________________________________________________________________ _______________________________________________________________________________________________________________________ _______________________________________________________________________________________________________________________ _______________________________________________________________________________________________________________________ _______________________________________________________________________________________________________________________ _______________________________________________________________________________________________________________________ _______________________________________________________________________________________________________________________ _________________________________________________ I have written the above statement and certify that it is true to the best of my knowledge. Witness Signature: _________________________________________________________________ Date:_______________________________ Reviewed by Investigator Signature: _____________________________________________________________ Date: _______________________________ Original—Accident Investigation File Brentwood Services Loss Control