Micro-organism Risk Assessment form
advertisement

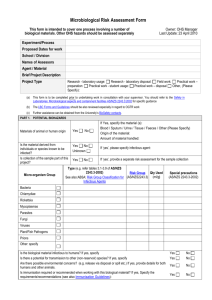
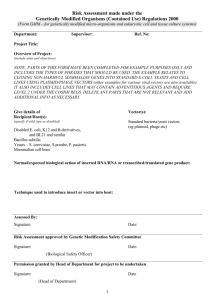
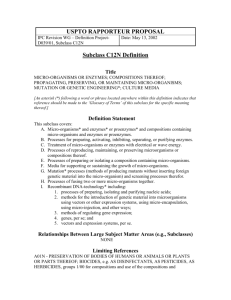
Faculty of Science Microbiological Risk Assessment Where space on this form is insufficient attach a separate sheet and indicate in appropriate place. This form is to be filled in by the subject coordinator in consultation with the laboratory manager. Please refer to AS/NZS 2243.3:2002 Safety in Laboratories Part 3: Microbiological aspects and containment facilities. If the work involves organisms of Risk Group 2 the Laboratory Manager will seek approval from the Biological Safety Committee (BSC) prior to commencement. Micro-organism Group Name of Micro-organism Bacteria Chlamydiae Rickettsiae Mycoplasma Parasite Fungi Virus Prion Risk Group Special Precautions (AS/NZS2243.3) (refer to AS/NZS 2243.3) -select-select-select-select-select-select-select-select- Do the micro-organisms produce infection in humans? yes no If yes, please specify: Are the micro-organisms highly infectious to humans? yes no yes no What level of containment is required? PC1 PC2 Are containment levels adequate? yes no Does the Biosafety Committee carry out an annual inspection of the laboratory? yes no Did the facility pass the annual inspection by the IBSC? yes no Will the micro-organisms be stored in the facility? yes no If yes, specify: Is immunisation required when working with these micro-organisms? If yes, specify the requirements: Containment Facilities If yes, when was the last inspection of the laboratory carried out by the IBSC? If yes, specify the storage requirements: Fridge Freezer Cold room Incubator Liquid Nitrogen bench Other: (please specify) Is there proper labelling of stored organisms? Microbiological Risk Assessment form V1 yes no Page 1 Procedures & Risk Controls What procedures will be used with the micro-organisms? (Please tick appropriate box) Aspiration Sonication Slide Preparation Vigorous Shaking/Mixing Pouring Pipetting Blending Grinding Centrifugation Using Automated Equipment Microbiological/Tissue Culture Other: Are there written procedures in case of accidents and/or spillage? yes no Is there appropriate equipment and supplies to cater for accidents and/or spills? yes no Are there adequate washing facilities available for use? yes no yes no yes no yes no Are there appropriate sterilisation/autoclave facilities available? N/A Are procedures for cleaning or laundering of protective clothing adequate? Is disposal/treatment of infectious material appropriate? List any specific disposal procedures: N/A Proposed Precautions and/or Controls List the protective devices intended to be used, including Personal Protective Equipment (PPE): Biological Safety Cabinet I Gown Disinfectant Biological Safety Cabinet II Face Mask Sharps Disposal Gloves Face Shield Other: N/A Is the Biological Safety Cabinet NATA certified annually? yes no Have the following factors been adequately considered? Safety Training yes no Legislative Standards yes no Job Specific Training yes no Supervision yes no Other (please specify): Special Approvals: Has approval been obtained from the following? Please attach as appropriate. Is approval required? Are documents attached? Institutional Biosafety Committee (IBSC) yes no yes no Office of the Gene Technology Regulator (OGTR) yes no yes no Australian Quarantine Inspection Service (AQIS) yes no yes no Other: yes no yes no Comments: Microbiological Risk Assessment form V1 Page 2 Actions / Comments: Remaining Risks: List of Attachments: 1 2 3 4 5 6 Risk assessment completed by: Name: Signature: Date: Name: Signature: Date: Name: Signature: Date: Name: Signature: Date: Name: Signature: Date: Consultation Signed (ALL persons involved in the project) Approvals and Comments: Name Signature Approval y/n Facility Manager -select- Head of School -select- Microbial Risk Assessment Page 3 of 3 Comments