Ethyl alcohol
advertisement

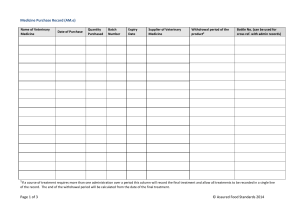
Managing Alcohol Withdrawal Syndrome Mercy Hospital & Trauma Center Janesville, WI Jenny Kleinert, BSW, BSN, RN-BC, PMHN jkleinert@mhsjvl.org Mercy Options: Inpatient Behavioral Health Unit – Psychiatry and Detox 608-756-6508 Frequently Used Terms Term Characteristics Alcohol abuse Alcohol dependence Alcohol withdrawal syndrome (AWS) Delirium tremens (DTs) Regular excessive use of alcohol with failure to meet responsibilities, such as work and family roles; Often drink during dangerous situations, such as driving or operating machinery; Legal problems occur secondary to alcohol use; Continue to drink in spite of effect on relationships; Need to drink more alcohol to achieve the same pleasurable effect Crave alcohol; Lose the ability to limit drinking; AWS occurs when abstinence occurs abruptly; Develop a tolerance for alcohol; Consume more alcohol than even intended when the individual began drinking; Numerous attempts to cut down or stop drinking; Always finding/drinking/recovering from alcohol; Give up/reduce activities because of drinking habits; Continue to indulge in alcohol in spite of being informed of the dangers to health and relationships Criterion A: Cessation or reduction of alcohol use that has been heavy and prolonged Criterion B: Two or more clinical manifestations that occur within hours or days of the last drink; Other medical or mental health problems are not the cause of the patient's manifestations The worst and severest form of AWS begins 48-96 hours after last drink, peaks at Day 5; Autonomic hyperactivity: tachycardia, tachypnea, hypertension, tremors, hyperthermia; Reduce clarity of surroundings; Memory deficit, disorientation, language Page 2 of 12 disturbance, and hallucinations; Perceptual disruption; Disturbances develop in a short period of time and fluctuate during the day A form of alcoholic psychosis characterized primarily by auditory hallucinations occurring in a clear sensorium, abject fear, Alcohol hallucinosis and delusions of persecution. The condition develops shortly after prolonged and heavy alcohol intake is stopped or reduced, usually within 48 hours. Usually a single seizure; Can occur in the absence of AWS or DTs; Generalized tonic-clonic Alcohol withdrawal seizures convulsions; Primarily occurs in patients with chronic alcoholism; If left untreated, may progress to DTs Due to thiamine deficiency; An acute life-threatening neurological Wernicke's syndrome disordered; Exhibited by paralysis of the eye muscle, nystagmus, and ataxi Due to thiamine deficiency; Manifested by inability to recall information, inability to assimilate Korsakoff's psychosis new information, decreased spontaneity, decreased initiative, and confabulation NOTE: Nurse's need to understand these terms in order to be proactive in managing the care of a patient who has a problem with alcohol. Page 3 of 12 The CAGE Questionnaire More than two positive responses to the questions suggest alcohol dependence and indicate further assessment is warranted. 1. 2. 3. 4. Have you ever felt you ought to Cut down on your drinking? Have people Annoyed you by criticizing your drinking? Have you ever felt Guilty about your drinking? Have you ever had a drink first thing in the morning to steady your nerves or to get rid of a hangover (Eye-opener)? Page 4 of 12 Symptoms of Alcohol Withdrawal Syndrome Time of occurrence after last alcohol use Symptoms 6 to 12 hours Minor withdrawal symptoms: insomnia, tremulousness, mild anxiety, gastrointestinal upset, headache, diaphoresis, palpitations, anorexia 12 to 24 hours (symptoms usually resolve within 48 hours) 24 to 48 hours (symptoms reported as early as two hours after cessation) 48 to 72 hours (symptoms peak at five days) Alcohlic hallucinosis: visual, auditory, or tactile hallucinations Withdrawal seizures: generalizaed tonicclonic seizures Alcohol withdrawal delirium (delirium tremens): hallucinations (predominately visual), disorientation, tachycardia, hypertension, lowgrade fever, agitation, diaphoresis Page 5 of 12 Effects of alcohol on the body and supportive care for patients with alcohol withdrawal syndrome System affected/ cancer risk Effect Mechanism Central nervous system Impaired judgement and memory Imparied balance and motor coordination Sleep disturbances Peripheral neuropathy Alcohol-related psychiatric disroders Dementia Depression Hallucinations Wenicke encephalopathy Korsakoff syndrom Cardiovascular Beneficial effects: Possible reduction in risk for death d/t cardiovascular conditions (1-2 drinks per day over long periods) Deleterious effects: Decreased myocardial contractility Cardiomyopathy Dysrhythmias Mild to moderate hypertension Hematopoietic Increased size of RBCs (mean corpuscular volume) Decreased production of WBCs Thrombocytopenia Nursing Interventions Maintain patient's safety Provide quiet Effects are due to the environment combination of the direct Have patient avoid toxic effects of alcohol on television and other neural tissue, thiamine activities that may definciency, and contribute to nutritional deficits hallucinations Initiate interventions to prevent falls Beneficial effects occur because alcohol increases levels of highdensity lipoprotein and decreases platelet aggregation Deleterious effects are due to the direct toxic effects of alcohol on cardiac muscle and the vasopressor effects of ethanol Monitoring patients for dysrhythmias Provide rest to reduce fatigue Monitor for hypertension Effects are due to the direct toxic effects of alcohol on bone marrow that cause suppression and malnutrition-related folate deficiency Monitor blood values and bleeding Do a complete nutritional assessment Encourage patient to eat nutritiously Maintain a safe environment and initiate Page 6 of 12 interventions to avoid injury Prevent infection Gastrointestinal Esophageal inflammation Mallory-Weiss lesions Esohphageal varices Acute pancreatitis Alcohol-induced hepatitis Cirrhosis Musculoskeletal Cancer risk Effects occur because alcohol stimulates an increase in acid production and causes direct damage of the gastric mucosal barrier; cirrhosis occurs as a result of fatty buildup in the liver Monitor patient for gastroentestinal bleeding Monitor for alterations in liver function Maintain a safe Effects on muscle tissue environment are due to the direct toxic effects of alcohol on Initiate interventions to muscle tissue. Skeletal prevent falls effects are due to the direct toxic effects of alcohol on osteoblasts Alcohol myopathy Lower bone density Increased risk for fractures Increased risk for caner of the Breast Esophagus Oral cavity Overall risk of cancer is 10 times greater in persons who are alcoholic than in the general popluation Alcohol is not a directacting carcinogen but one of its metabolites, acetaldehyde, may act as a tumor promoter. Chronic alcohol use also causes increased degradation or retinol by the liver and results in vitamin A deficiency, which is associated with an increased incidence of cancer Page 7 of 12 Explain effects of chronic alcohol use Offer information on treatment options and sources of support Medications Frequently Used for AWS Benzodiazepines Examples: o lorazepam (Ativan), Only benzodiazepine recommended for IM administration (d/t erratic absorption of other agents administered the same route) o chlordiazepoxide (Librium), o valium (Diazepam) Recommended over other medications because they have better documented efficacy, are safer, and are less likely to lead to abuse o The potential for abuse is higher with benzodiazepines with a rapid onset of action, than it is for those with a slower onset of action Reduces the severity of alcohol withdrawal, including the incidence of delirium and seizures Dosage should be individualized, based on severity of withdrawal (as indicated by the withdrawal scale score, or CIWA-Ar) NOTE: Other medications may be used to treat alcohol withdrawal but are not recommended as monotherapy, they should be used in combination with benzodiazepines. Vitamins Example: thiamine (Vitamin B) o Essential nutrient to all tissues of the body for carbohydrate metabolism o Suggested dosing: 50-100mg PO qday X 3-7days (or until treatment of alcohol withdrawal ends) Corrects deficiencies Prevents Wernicke-Korsakoff syndrome Alpha-adrenergic agonists Example: clonidine (Catapres) Studies show that this may help alleviate symptoms in patients with mild to moderate alcohol withdrawal o Effect on rate of delirium and seizures is unknown Anticonvulsants Examples: valproic acid (Depakote), cabamazepine (Tegretol), gabapentin (Neurontin) Research supports use to prevent seizures related to alcohol withdrawal Beta-blockers Examples: atenolol (Tenormin), propranolol (Inderal) Adjunctive therapy o May be useful for patient’s with co-morbid conditions (i.e. – coronary artery disease) Neuroleptics Examples: chlorpromazine (Thorazine) or haloperidol (Haldol) May reduce symptoms related to alcohol withdrawal, but are significantly less effective than benzodiazepines May be indicated for severe agitation, thought disorders, or hallucinations Page 8 of 12 NOTE: when used alone, risk for seizure increases and delirium is unchanged Ethyl alcohol ***Not recommended. There is little evidence to support its use OR prove that it is safer and/or more effective than the use of benzodiazepines. Miscellaneous (NOTE: The following medications should only be initiated once withdrawal is resolved and the patient intends on abstaining from continued alcohol use.) disulfiram (Antabuse) o Used to deter relapse o Produces adverse symptoms (when mixed with alcohol) Violent throbbing headache Nausea and vomiting Chest pain Palpitations Breathlessness Flushed face Tachycardia Arrhythmias Decrease BP leading to vertigo, blurred vision, and possible collapse o Reaction can occur within 10 minutes of consuming alcohol o Very small amounts can induce reaction (medications – cough mixtures, mouthwashes, foods) o Only useful for those individuals intending on abstaining from alcohol indefinitely acamprosate (Campral) o Reduces craving for alcohol o Therapy recommended for 6-12 months naltrexone (Depade) o Opioid antagonist Blocks the effects of the body’s natural opioid-like substances (endorphins) Inhibits the pleasant feelings associated with alcohol use overtime it breaks the association between pleasure and alcohol in the brain ***NOTE: This medication will block ALL other opioid analgesics!!! Page 9 of 12 Benzodiazepines Most Commonly Used for the Effective Management of Alcohol Withdrawal Ativan Route P.O. I.V. I.M. (lorazepam) Onset Peak 1 hr 2 hr 60-90 5 min min 60-90 15-30 min min (chlordiazepodie Librium hydrochloride) Route Onset Peak P.O. Unknown 1/2-4 hr Valium Route P.O. (diazepam) Onset Peak 30 min 2 hr I.V. I.M. P.R. 1-5 min Unknown Unknown 1-5 min 2 hr 90 min Page 10 of 12 Duration 12-24 hr 6-8 hr 6-8 hr Duration Unknown Duration 20-80 hr 15-60 min Unknown Unknown References American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th ed., text rev.). Washington, D.C. Burton, J. (2010). Alcohol withdrawal syndrome. MedSurg Matters!, 19(5), 7-12. Compton, P. (2002). Caring for an alcohol-dependent. Nursing2002, 32(12), 58-63. Doyle, L., Keogh, B., & Lynch, A. (2010). Pharmacological management of alcohol dependence syndrome. Mental Health Practice, 14(1), 14-19. Kelly, A., & Saucier, J. (2004). Is your patient suffering from alcohol withdrawal?. RN, 67(2), 27-32. Keys, V. (2011). Alcohol withdrawal during hospitalization. The American Journal of Nursing, 111(1). 40-44. McKinley, M. (2005). Alcohol withdrawal syndrome: Overlooked and mismanaged?. Critical Care Nurse, 25(3), 40-49. Molnar, A. (2006). One drink over the line. Nursing2006 Critical Care, 1(6), 20-33. Videbeck, S. (2008). Psychiatric-mental health nursing, 4th Ed. Philadelphia, PA: Lippincott Williams & Wilkins. Vincent, W., Smith, K., Winstead, S., & Lewis, D. (2007). Review of alcohol withdrawal in the hospitalized patient: Diagnosis and assessment. Orthopedics, 30(5), 358-361. Vincent, W., Smith, K., Winstead, S., & Lewis, D. (2007). Review of alcohol withdrawal in the hospitalized patient: Management. Orthopedics, 30(6), 446-449. Page 11 of 12 NOTES ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ Page 12 of 12