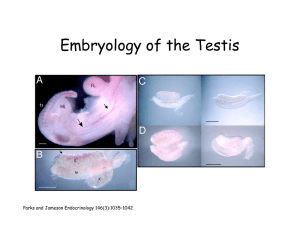
At about the 28th week of gestational age, the testes begin descent
advertisement

At about the 28th week of gestational age, the testes begin descent through the internal inguinal ring, ultimately ending up in the scrotum. The left testis starts earlier than the right, and full descent may not be complete until several months after birth. Adequate amounts of male hormone are necessary for testicular descent. Inadequate levels of male hormone or poor end- organ response to the hormone can interrupt this process resulting in an undescended testis (UDT), either unilateral or bilateral . The UDT can be found anywhere from the level of the kidney in the retroperitoneum to the external inguinal ring, although it most commonly resides in the inguinal canal. A congenital indirect inguinal hernia or patent processus vaginalis is associated with the UDT 90% of the time. Occasionally a testis is totally absent, presumably due to antenatal torsion with resorption. The incidence of UDT in full-term boys by one year of age is about 0.5%. Premature baby boys have an incidence 10 times higher. Fifty per cent of UDT occur on the right and 25% on the left, and 25% are bilateral. This distribution is similar to that of congenital inguinal herniae and reflects the order of testicular descent. UDT is diagnosed by physical examination. The examination must be conducted carefully and compulsively with warm hands in a relaxed cooperative patient so as to distinguish the retractile testis from the true UDT. Starting at the internal inguinal ring in the upper outer groin, firm downward pressure is used along the inguinal canal to locate the testis and attempt to push it into the scrotum. If the testis can be brought down into the scrotum, it is a retractile testis and not an UDT. Such retractile testes will ultimately end up in the scrotum on their own when endogenous androgenic hormone levels increase, and operation is not indicated. If a testis cannot be palpated at all, it is likely either intraabdominal or absent. Indications for operation for UDT include the following: 1. Enhanced spermatogenesis/fertility: Above the scrotum, the UDT is subjected to higher body temperature. Testicular damage is related to the duration of exposure to and the magnitude of the higher temperature; these two factors correlate to the age at orchiopexy and the level of descent, respectively. An autoimmune reaction may occur which can also affect the contralateral descended testis in cases of unilateral UDT. Pathologic changes (eg, decrease in spermatogonia, decrease in tubular diameter) begin to appear in the second or third year of life. I generally advise operation after one year of age to allow the testis that might further descend to do so but before age two to avoid testicular damage. Left uncorrected, 37% to 70% of patients with unilateral and 100% with bilateral UDT are infertile. With early repair, 95% of boys with unilateral and 70% with bilateral UDT will achieve fertility. 2. Monitoring for malignancy: Testicular cancer is 40 times more common in patients with UDT compared to the general male population. Unfortunately, orchiopexy does not reduce the incidence of malignancy, but it makes the testis easier to examine, presumably leading to earlier detection. 3. Decreased risk of trauma or torsion: The abnormally positioned UDT is more prone to trauma or torsion, and orchiopexy decreases this risk. 4. Cosmetic/Psychologic considerations. Preoperative counseling of the parents of a boy with UDT is very important so that they understand the goals and limitations of surgery. A testis may not be present, or if present, it may not be salvageable. In addition, injury may result to the testis or associated structures during operation. Neither general growth and development nor development of secondary sexual characteristics are affected by testicular position. Orchiopexy for a palpable UDT involves an inguinal exploration to mobilize the spermatic vessels and vas deferens to allow the testis to be brought down into the scrotum. Any associated hernia is repaired appropriately. The scrotum is stretched, and the testis is secured in the deep scrotum, most commonly with a dartos pouch technique in which the testis is anchored in a space developed between the dartos fascia and the scrotal skin. I find laparoscopy helpful in patients in which the UDT is not palpable in the groin. If the vas and spermatic vessels end blindly, this proves that the testis is absent, and the operation can be concluded immediately. In the case of an atrophic or very high intra-abdominal testis, an orchiectomy can be performed if a normal testis is present contralaterally. With a low intra- abdominal testis near the internal inguinal ring, if it can be mobilized sufficiently, a formal orchiopexy can be performed at the same time; if the vascular pedicle seems too short, a two- stage Fowler-Stephens approach can be used in which first the spermatic vessels are divided in the high retroperitoneum at laparoscopy, and then 6 to 12 months later, after a collateral blood supply has developed, an orchiopexy via an inguinal approach can be performed. Possible complications following orchiopexy include injury to the vas (1%), injury to the spermatic vessels leading to testicular atrophy (1% to 8%), and retraction of the testis out of the scrotum (5% to 10%). In summary, I would like to reiterate a few key points. Retractile testis must be differentiated from UDT to avoid unnecessary operation. Although ample time should be allowed for full testicular descent to occur, orchiopexy should be performed in a timely fashion after the first birthday to avoid long-term damage to the testis. In the case of nonpalpable UDT, laparoscopy offers a minimally invasive approach to diagnosis and treatment. Dr. Breaux is a pediatric surgeon and surgical critical care specialist practicing in Grand Junction, Colorado.