Texas ACEP round the horn cases
1. 49 year-old male with palpitations. No significant PMH and reports “heart racing” with an onset
12 hours ago. No reports of chest pain, syncope, or any complaint of shortness of breath. Exam
is unremarkable with the exception of irregular heart rate and 12 lead shows atrial fibrillation
with a rate of 105. Our patient does report that he is not a smoker but does drink socially. There
is no significant past family history.
Our clinical questions
Should we rate control and admit?
Should we cardiovert and discharge?
If we cardiovert should we use electricity or chemical?
If we cardiovert should we start any anticoagulants?
Do we need to get a TTE or TEE prior to cardioversion?
What if the patient had >48 hours of symptoms?
Study #1: Wyatt W. Decker, et al. A Prospective, Randomized Trial of an Emergency
Department Observation Unit for Acute Onset Atrial Fibrillation. Annals of Emergency
Medicine, 2007
Study #2: Von Besser, Kiera, et al. Is Discharge to Home After Emergency Department
Cardioversion Safe for the Treatment of Recent-Onset Atrial Fibrillation. Annals of Emergency
Medicine, December 2011.
Study #3: Ian G. Stiell, et al. Association of the Ottawa Aggressive Protocol with rapid discharge
of the emergency department patients with recent-onset atrial fibrillation or flutter. Canadian
Journal of Emergency Medicine, 2010
Study #4 Vinson et al. Managing Emergency Department Patients with Recent Onset Atrial
Fibrillation. The Journal of Emergency Medicine, Vol. 42, No. 2, pp. 139–148, 2012
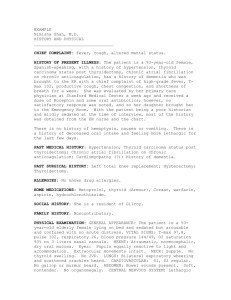
Case 2
46 year-old male presents with chest pain. History is 3 hours of intermittent sub-sternal chest
pain, associated anxiety and shortness of breath. He is currently chest pain free. There is no
significant PMH, and he denies any illegal drug use. There is no family history of CAD in men
under 50. His initial exam and diagnostic studies are unremarkable including a non diagnostic
ECG and initial CK, CK-MB and Troponin I?
Clinical questions:
What is his risk of ACS as the cause of his symptoms?
Does he need any further testing?
Can we exclude MI with his initial work up?
Can we exclude unstable angina?
Is he appropriate for discharge after his initial testing?
What management strategy should we use?
Study #1: Fesmire F, et al. Serial creatinine kinase (CK) MB testing during the emergency
department evaluation of chest pain: Utility of a 2-hour ΔCK-MB of +1.6 ng/mL. American Heart
Journal. 1998; 136(2): 237-244
Study #2: Fesmire et al. “Delta Creatinine Kinase-MB Outperforms Myoglobin at Two Hours
During Emergency Department Identification and Exclusion of Troponin Positive Non-STSegment Elevation Acute Coronary Syndromes the” Annals of Emergency Medicine
2004;44:12-19.
Study #3 Kline JA, Johnson CL, Newgard CD, et al. Use of computer-assisted attribute matching
to estimate pretest probability. Accad Emerge Med 2003May;10(5):509.
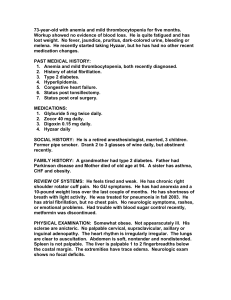
Case #3
42 year-old woman presents with a severe bilateral headache. She describes the onset as sudden
while sitting at her desk at work. There is no associated fever or neurologic deficits on her exam.
She does have a history of anxiety and migraine headaches. Her current headache is moderate to
severe in nature at this time. Her complete neurologic exam is normal.
Clinical questions:
Does she need any neuroimaging?
Does she need a lumbar puncture?
Can we substitute CT/CTA strategy to replace the CT/LP strategy?
If we have a traumatic tap is there any evidence to suggest if this can be differentiated from SAH
blood?
What therapy is first line?
Can we infer benign headache if our patients respond to analgesic therapy?
Study #1: Nijjar, MD, et al. Computed Tomographic Angiography as the Primary Diagnostic Study
in Spontaneous Subarachnoid Hemorrhage. J Neuroimaging 2007;17:295?299
Study #2: Carstairs et al. Computed Tomographic Angiography for the Evaluation of Aneurysmal
Subarachnoid Hemorrhage. Academic Emergency Medicine 2006; 13:486–492
 0
0