References
Describing
Rotator Cuff
Tears: For the
Sonographer
Bianchi S and Martinoli C, 2007. Ultrasound of the Musculoskeletal
System. Springer.
Frank RM, Chahal J and Verma NN, 2013. Partial-Thickness Rotator Cuff
Tears. Shoulder Arthroscopy, 277-287
McNally E, 2005. Practical Musculoskeletal Ultrasound. Elsevier Churchill
Livingstone
Saccomanno MF, Salvatore M, Grasso A and Milano G, 2013. Full-thickness
Rotator Cuff Tears. Shoulder Arthroscopy, 289-306
Tse AK, Lam PH, Walton JR et al, 2015. Ultrasound Determination of
Rotator Cuff Tear Repairability. Shoulder and Elbow
1.
Grading and classifying rotator cuff tears can be
challenging for the novice. This pamphlet aims to
highlight the differentiating factor and key point
accompanied with annotated sonographic images.
Caitlin Gardiner
16271216
CAITLIN GARDINER
Shoulder Tear Basics
When describing the position of the tear within the supraspinatus. It
is useful to use the bicep tendon as a landmark, as figure two
demonstrates.
Rotator cuff tears are the most commonly encountered shoulder disorder
(Saccomanno). Ultrasound demonstrates good sensitivity and specificity in
detection of rotator cuff tears (bianchi). Accurate tear assessment is important as
it strongly impacts treatment and surgical repairability (Tse).
Prior to classifying tears, it is important to understand the appearances of a
healthy rotator cuff. Figure shows the appearance of a healthy tendon, indicating
the bursal and articular surface, bony insertion and tendinous fibrillary pattern.
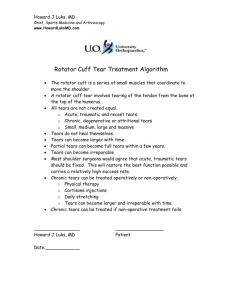
Fig Two: A short-axis image of a left healthy supraspinatus. The bicep
tendon is clearly visible (red) allowing accurate location of the
anterior, mid and distal portions of the supraspinatus tendon.
There are several secondary signs to aid the detection of rotator cuff
tears.
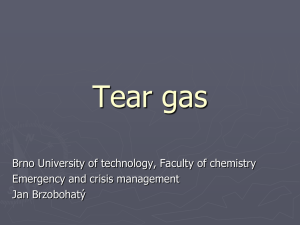
Fig One: A long-axis healthy supraspinatus in an 18-year old female. A regular fibrillary pattern is noted
Fluid in the bursa can help outline the margin of a tear
between the bursal surface (red) and the articular surface (yellow). No bony irregularity is seen at the
Focal thickening of the bursa may indicate an adjacent
insertion interface (green lines).
tear
Flattening of the bursa arch is suggestive of a significant
When classifying a rotator cuff tear, a sonographer is expected to describe:
tear
Bony irregularity or enthesopathy may indicate a tear
The tendon the tear is located within
The position within that tendon
The extent of the tear
-Full thickness (Complete/Incomplete)
-Partial thickness (Bursal/Articular/Intrasubstance)
The size of the tear
The extend of any retraction
Whether the tear is associated with tendinopathy or not
Factors of rotator cuff tears include
Age (decreased cellularity and vascularity)
Decreased vascularity( relative hypovascularity of the
articular side of the cuff, especially anterior supraspinatus)
Subacromial Impingement (often results in bursal surface
tears)
Internal Impingment (repetitive contact between the
posteriorsuperor glenoid and undersurface of the cuff)
Trauma (Frank)
Full Thickness Tears
Full thickness tears extend between the bursal and articular surface
and can be degenerative (mean age of 65) or traumatic (mean age of
55). Traumatic tears are typically caused by trauma on abduction
on an externally rotated arm Patients will typically present with
pain, though only 1/3 of full-thickness tears are symptomatic. Most
commonly, full-thickness tears of the rotator cuff occur in the
anterior third of the supraspinatus or the near the junction of the
supraspinus and infraspinatus. (saccomano)
A full-thickness tear should be further classified
as full-width/complete or partialwidth/incomplete. Measure the width of tear in
the short axis and the retractrion in a longaxis.
Ultrasound Findings
4
A thin hypoechoic cleft connecting the joint cavity and the bursa, evident
in both long and short axis
In the presence of a joint effusion, the tear will appear as a focal
hypoechoic area
A focal area of inability to visualize tendon fibres
Depending on size of the tear, there may/may not be a retraction of fibres
A focal bursal thickening
Full-thickness tears of the supraspinatus typically occur in the anterior
third of the tendon
Significant full thickness tears will show a bear humeral head
Typically bone irregularity
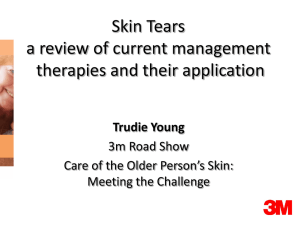
Fig: A long and short axis images of the right supraspinatus of a 90 year old female. A full-thickness tear is
noted in two-planes, characterized by the lack of visible tendon fibres and hameatoma within. The bicep
tendon is noted in the transverse plane which allows confident location of the tear within the supraspinatus.
Fig: A short and long axis of the mid and posterior fibres, respectively, of a right supraspinatus of a 59
year old male. A full thickness tear expanding 21mm is noted with retraction of fibres 19mm. Care must
be taken not to classify this a complete tear, as when scanning in the longitudinal place, some fibres are
seen posteriorly.
Fig: Short and long-axis images of the supraspinatus in a 24 year old female with recent trauma. A
6*5mm full-thickness tear is noted of the mid-fibres. A focal hypechoic area without the presence of
tendon fibres is noted expanding from the bursal to the articular surface, with adjacent bony
irregularity. Flattening of the bursa is noted superficial to the tear in the long-axis.
1
Partial Thickness Tears
What to Include?
Approximately 13-18% of rotator cuff tears are described as partialthickness tears and typically occur in a younger population compared to
full-thickness tears (Bianchi). Partial thickness tears are common due to
age-related metabolic and vascular changes or a result of stress, be it
acute or chronic micro-trauma. Degenerative partial-thickness tears
typically affect the anterior supraspinatus, whilst trauma-related tears
more commonly affect the supraspinatus/infraspinatus junction
(Frank).
Fig: Long and short axis images on the left supraspinatus of a 23 year old female. A 4*5mm focal
hypoechoic area with a lack of tendon fibres is noted in both planes. The tear involves the articular
surface and does not extend to the bursal surface, classifying it as a partial thickness tear. The bicep is
noted in the transverse plane, indicating the tear is located in the anterior portion of the supraspinatus.
Measure a partial thickness tear in two-planes or as a
percentage of the tendon diameter. Classify the tear as
bursal or articular surface.
Ultrasound Findings
Ultrasonic findings include
A localized hypoechoic area, affecting only part of the tendon thickness
A cleft or defect is noted in both the long and short-axis, and still present with a
change of transducer tilt
May involve either the BURSAL or ARTICULAR surface (articular are more common)
Typically occur in the anterior third of the supraspinatus
A bursal surface tear may demonstrate fluid herniation into the tear
Fig: Long and short axis images of a 56 year-old male right supraspinatus. An 8*6mm partial-thickness tear of
the anterior fibres, involving the bursal surface, is noted with diffuse tendinopathy. A focal hypoechoic area
without tendon fibres is noted, with tendon fibres noted deep to the region. A slight depression of the bursa
can be appreciated.
Articular surface appear as a deep mixed hyperechoic/hypoechoic foci at the
hummeral neck, due to separation of the retratcted distal segment, resulting in a
new interface. Often accompanied with bny irregualrities in the greater tuberosity
2
Fig: A long-axis image of the right subscapularis in a 66-year old male. An 8mm partial-thickness involving the
bursal surface is noted of the superior fibres.
3
Complete and Massive
Tears
When a full-thickness involves the full-width, it is known as a complete or
massive tear, and results in retraction of the tendon. The tendon tip may be
noted in acute ruptures, but typically will retract beyond the caracoacromial
arch with time.
Ultrasound Findings
No notable tendon fibres
A naked humerus
Marked irregularity of the cubchondral cortex and humeral head
cortex (McNally)
A massive tear of the supraspinatus is closely related with massive
tears of the infraspinatus and subscapularis
Infraspinatus and subscapularis atrophy is also closely related with
supraspinatus tears
Fig: Long and short axis images of left supraspinatus in 78 year old female. A
complete tear is noted with 26mm posterior retraction of fibres. No tendon
fibres are visible and complex haematoma covers the greater tuberosity.
Marked bony irregularity is noted. This patient also demonstrated a complete
subscapularis rupture and a bursal effusion.
Intra-substance Tears
Intrasubstance tears occur more commonly in older
generation, with degeneration a more significant cause
than trauma (McNally).
Ultrasound Findings
Subtle, thin, fluid-filled, intra-tendinous longitudinal splits
Oriented from the bony surface without involving either the
bursal or articular surface
May be surrounded by a hypoechoic halo of fluid or
edematous tendon- known as a ‘rim rent’ tear
Typically better appreciated in a short-axis
 0
0