Dr. Sandeep S
advertisement

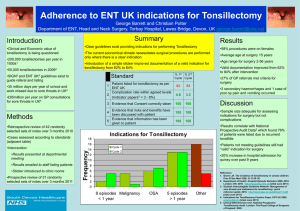
ORIGINAL ARTICLE QUINSY TONSILLECTOMY- A SAFE PROCEDURE. Sandeep. S, T. Shivram Shetty, Prakash B. G. 1. 2. 3. Assistant Professor. Department of ENT, JSS Medical College and Hospital, Mysore. Professor & HOD. Department of ENT, JSS Medical College and Hospital, Mysore. Associate Professor. Department of ENT, JSS Medical College and Hospital, Mysore. CORRESPONDING AUTHOR: Dr. Sandeep S Door no .74, Brindavan Extension, 1st stage, 3rd Cross, Mysore-20. E-mail: drshetty79@yahoo.co.in Ph: 0091 9845366551. ABSTRACT: A Peritonsillar abscess (quinsy) is collection of pus between Fibrous capsule of Tonsil usually at it upper pole and superior constrictor muscle of pharynx. There are different modes of treatment of peritonsillar abscess. The most common mode of treatment is incision and Drainage followed by in interval tonsillectomy 4 to 6 wks later, The other methods of treatment are Needle aspiration and ABSCESS TONSILLECTOMY/HOT TONSILLECTOMY/ QUINSY TONSILLECTOMY, Which has become popular during recent years. This method of doing tonsillectomy during acute, Infective stage is also known as “TONSILLECTOMY A CHAUD” We did a study in our hospital to evaluate the advantages associated with abscess tonsillectomy done under General anaesthesia by Dissection and Snare Method .The Parameters Considered was Primary, Secondary and Reactionary Hemorrhage, Post-OP pain, Duration of Hospitalization and any other complications associated with procedure. KEY WORDS: Quinsy, Tonsillectomy, Abscess, Secondary Hemorrhage. INTRODUCTION Peri tonsillar abscess is the most common deep space infection of the head and neck region that occurs commonly in adults and is typically caused by combination of aerobic and anaerobic bacteria. A peritonsillar abscess (quinsy) is collection of pus between Fibrous capsule of Tonsil usually at it upper pole and superior constrictor muscle of pharynx. Two mechanisms have been proposed to explain development of peritonsillar abscess. One is by direct spread of an inadequately treated acute tonsillitis, where the infection directly spreads to peritonsillar space and results in peritonsillar cellulitis and abscess. Second mechanism is an abscess formed in a group of salivary glands in supratonsillar fossa known as WEBER GLANDS These group of salivary glands are located in superior tonsillar pole and there ducts secrete through tonsillar fossa, If there is tonsillar disease, chronic tonsillitis etc. There may be obstruction to ducts of Weber glands that can lead to stasis of secretions which in turn leads to bacterial colonization and bacterial infection. There are different modes of treatment of peritonsillar abscess. The most common mode of treatment is incision and drainage followed by in interval tonsillectomy 4 to 6 wks later, this type of tonsillectomy is designated as “TONSILLECTOMY A FROID” The other methods of treatment are Needle aspiration and ABSCESS TONSILLECTOMY / HOT TONSILLECTOMY /QUINSY TONSILLECTOMY, Which has become popular during recent Journal of Evolution of Medical and Dental Sciences/ Volume 2/ Issue 10/ March 11, 2013 Page-1447 ORIGINAL ARTICLE years. This method of doing tonsillectomy during acute, Infective stage is also known as “TONSILLECTOMY A CHAUD” The risks of abscess tonsillectomy are mainly theoretical and none of the studies showed increased incidence of secondary hemorrhage and spread of infection. This study aims at evaluating the advantages and disadvantages associated with immediate abscess tonsillectomy. METHODOLOGY: SOURCE OF DATA: Patients with peritonsillar abscess visiting JSS Hospital ENT OPD period of study between 2008 and 2011. METHODS OF COLLECTION OF DATA: Data was collected in a pretested proforma which meets the objective of the study 30 cases was selected from the total number of cases by using simple random sampling method. The analysis will be done using parameters the mean, the standard deviation, standard error, T-test and chi-square test. 5% or 0.5 and 1.1 or 0.01 levels of significance will be considered for the purpose of comparison at the specified degree of freedom. INCLUSION CRITERIA: Patients with Unilateral peritonsillar abscess only are included in study. Patients above 6 yrs are included, As tonsillectomy is usually not done below 6yrs of age EXCLUSION CRITERIA: Patients below 6 yrs and above 45 yrs are excluded. Patients with chronic ailments like diabetes mellitus, hypertension, asthma, epilepsy and bleeding diathesis are excluded. Patients having peritonsillar abscess associated with dental infections, nasal and ear pathology are excluded. METHOD OF STUDY: To interview the patients before abscess tonsillectomy and case history collection. To assess the general condition of patient and carry out all routine investigations. To administer pre operative antibiotics that is Third generation cephalosporin’s (Cefotaxim 30mg/kg) and metronidazole (500mg 8th hourly) intravenously to cover both aerobic and anaerobic infections and anti-inflammatory drugs and analgesics to reduce pain and inflammation. To carry out abscess tonsillectomy using dissection and snare method. To measure preoperative bleeding and to look out for any post operative bleeding from tonsillar fossa. To assess the pain following procedure. Post operative pain is assessed on basis of Objective Pain Scale (OPS) which is a validated 1-10 scale for assessment of post operative pain. The parameters used for assessment are Blood pressure, movement, posture, verbal complaint and agitation and in case of children’s crying is taken into account, According to OPS post operative pain is classified as No pain, mild, moderate and severe. 1 week and 4 weeks following procedure post operative follow up is done. To take into account any complications associated with the procedure. Journal of Evolution of Medical and Dental Sciences/ Volume 2/ Issue 10/ March 11, 2013 Page-1448 ORIGINAL ARTICLE STASTICAL METHOD EMPLOYED: Following statistical methods were employed in the present study Frequencies/Descriptives Chi-square test Contingency coefficient (Cross Tabs) One-way ANOVA (Analysis of variance) RESULTS: Majority of the cases belonged to age group between 35-46yrs of age and the cases were predominantly found in Males The culture report of pus collected during the procedure showed Mixed growth in majority of cases Indicating that complete evacuation of pus is not possible with single sitting of incision and drainage and required repeated dilatations to evacuate pus completely. The incidence of primary haemorrhage and reactionary haemorrhage was nil in the cases studied, Even though the bleeding was more during surgery due to Acute inflammation but was not alarming or uncontrollable (usually between 80-120ml). Secondary haemorrhage was reported in only two cases usually between 4-6th day after surgery and was treated conservatively. This study showed that incidence of secondary haemorrhage is not as high as given in some literature. Objective pain scale (OPS) showed that pain during post operative period was of moderate degree and comparable with pain associated with regular and interval tonsillectomy. The mean total period of hospitalization was 3.82 days indicating the cost-effectiveness of treatment. Overall results of study of Abscess tonsillectomy showed that the procedure can be carried out safely without any greater risk of haemorrhage or other complications and was most cost effective method of treatment in draining the Abscess completely, preventing recurrence and decreasing total period of hospitalization. DISCUSSION: Of the 35 Cases studied, Most of the cases (17 accounting to 48.6%) were in the age group of 26-36yrs and least only 2 cases accounting to 5.7% in the age group of 6-15yrs. The mean age among Males Was 32.04 with a standard deviation of 8.46yrs and the mean age among females was 27yrs with a standard deviation of 7.97yrs the minimum age was 9yrs in males and 13yrs in females and the maximum age was 45yrs in males and 35yrs in females. The mean age of all the cases together was 30.46yrs with standard deviation of 8.53yrs. Out Of 35 cases 24 were males and 11 were females Out of all the cases studied 22 cases had Lt sided peritonsillar abscess and 11 cases had RT sided peritonsillar abscess. The routine investigations carried out in the patients showed elevated Total leukocyte count other investigations were within limits. All the cases were treated with pre operative antibiotics and analgesics and the surgery was carried out within 24hrs of admission. The incidence of primary and reactionary haemorrhage was Nil, Even though there was excessive bleeding during the procedure as compared to regular tonsillectomy it was not drastic or alarming and the amount of Bleeding was usually between 90-120ml. Secondary haemorrhage was seen in 2 out of 35 cases accounting to 5.7% and was usually observed between 4-6th post operative days both the cases were treated conservatively. Post operative pain assessment was done on basis of OPS (Objective pain scale) and most of the cases that is 65.7% of cases (23cases) showed moderate degree of pain Journal of Evolution of Medical and Dental Sciences/ Volume 2/ Issue 10/ March 11, 2013 Page-1449 ORIGINAL ARTICLE Severe pain was seen in only in 11.4% of cases (4 cases) these cases were treated with commonly used analgesics (NSAID’S). The other minor complications such as injury to posterior pillar (2 cases) and symptomatic lingual tonsil hypertrophy in 1case were seen. The average total period of hospitalization was 3.82 days with 3 days seen in 42.9% of cases and 4 days seen in 45.7% of cases the maximum period of hospitalization was of 8days seen in 1case of peritonsillar abscess with neck space infection. There was Non significant association between number of days of hospitalization and other parameters like haemorrhage, pain, other complications, age and sex. The culture analysis of the pus collected showed mixed growth in 20cases that is 57.1% of cases and anaerobic growth in 7 cases accounting to 20% of cases gram positive cocci was seen in about 17% of cases with B-hemolytic streptococci seen in most of the cases (11.4%).The cases were treated with combination antibiotics of cephalosporin’s and metronidazole post operatively. The study showed that the procedure Abscess tonsillectomy can be carried out safely without much complications and the incidence of secondary haemorrhage was not as high as compared to literature. BIBLIOGRAPHY: 1. J. Laryngol Otol 1981 Aug; 95(8): 805-7. Nielsen VM, Greisen O, Peritonsillar abscess II cases treated with tonsillectomy a chaud. 2. Laryngoscope, 1981 Aug; 91(8): 1226-30. Holt GR, Tinsley PP Jr. Peritonsillar abscess in children. 3. Acta Oto Rhinolaryngology Belg 2000; 54 (4): 459-64. Brojendian S, Bisschop P. Clinical advantage of abscess tonsillectomy in peritonsillar abscess. 4. Schweiz Med Wochenzchi 2000; Suppl 125; 175-195. Clerc S, Soldati D, Socio economic aspects in therapy of peritonsillar abscess. 5. Auris Nasus Larynx 2001; Nov 28 (4): 323-7. Jochen P, Windfuhr, Chen YS. Immediate abscess tonsillectomy – A safe procedure? 6. Clinical otolaryngology 2003 Oct; 28 (5): 420-4. Dunne AA, Granger O, Folz BJ, Sester Lenn A, Werner JA. Peritonsillar abscess – critical analysis of abscess tonsillectomy. 7. J Laryngol Otoal. 1992 Nov; 106 (11): 986-8. Chowdury CR, Bricknell MC. The management of quinsy – a prospective study. 8. Aurius Nasus Larynx 1999 Jul; 26(3): 299-304. Suzuki M, Veyama T, Mogi G. Immediate tonsillectomy for peritosillar abscess. 9. BMJ 2001 322: 943-5. Sculpher M, Drummond M, O’Brien B. Abscess tonsillectomy effectiveness and efficiency. 10. J. Laryngol Otol 1995 Dec 97(12): 1105-9. Mc Curdy JA Jr. Peritonsillar abscess – A comparison of treatment by immediate tonsillectomy and interval tonsillectomy. 11. Acta otolaryngology suppl. 1979; 360:67-9. Harma RA, Juola E, Ruoppi P, Vartiainen E.Abscess tonsillectomy a tiede. 12. J. Otol 1990; 19: 226-9 Hall S.F-Peritonsillar abscess: The treatment options. 13. Laryngoscope 1995; 105: 1-17 Herzon F.S Peritonsillar abscess: incidence, current management practices and a proposal for treatment guidelines. Journal of Evolution of Medical and Dental Sciences/ Volume 2/ Issue 10/ March 11, 2013 Page-1450 ORIGINAL ARTICLE a) Right Sided Quinsy b) Pus coming out on incision AGE -WISE DISTRIBUTION OF CASES No. of patients 12 10 8 6 4 2 0 6-15 16-25 26-36 Age groups 36-45 Male Female Journal of Evolution of Medical and Dental Sciences/ Volume 2/ Issue 10/ March 11, 2013 Page-1451 ORIGINAL ARTICLE INCIDENCE OF HEMORRHAGE No. of patients 35 28 21 14 7 0 PH RH SH Complications Presen t PH- Primary Hemorrhage RH- Reactionary Hemorrhage SH- Secondary Hemorrhage Graph showing Objective pain scale Journal of Evolution of Medical and Dental Sciences/ Volume 2/ Issue 10/ March 11, 2013 Page-1452 ORIGINAL ARTICLE 5.70% 2.90% NIL 91.40% INJURY TO POST.PILLAR LINGUAL TONSIL HYPERTROPHY Graph showing incidence of other complications 16 No. of patients 12 8 4 0 d3 d4 d5 Days d7 d8 Distribution of cases according to days of hospitalisation Journal of Evolution of Medical and Dental Sciences/ Volume 2/ Issue 10/ March 11, 2013 Page-1453