Nuclear Medicine Session - Society for Pediatric Radiology
advertisement

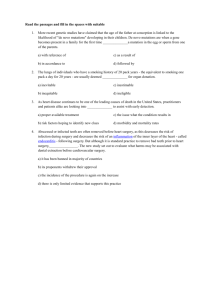
SPR 2014 Nuclear Medicine Session May 17, 2014 SAM Questionnaire Communicating with Parents and Referring Clinicians S. Ted Treves, MD 1. Compared to contrast agents used in CT and MRI, the administered volume and mass of 99mTc-MDP solution is A. 99mTc-MDP volume is approximately equal to CT and MRI contrast agents B. 99mTc-MDP volume is 2 times greater than CT and MRI contrast agents C. 99mTc-MDP volume is 20-200 fold less than CT and MRI contrast agents D. The masses of material injected are equivalent among 99mTc-MDP, CT and MRI contrast agents E. The mass of 99mTc-MDP administered material is greater than the mass from CT and MRI contrast agents Correct Answer: C References 1. Treves ST, Baker A, Fahey FH, Cao X, Davis RT, Drubach LA, Grant FD, Zukotynski K. Nuclear Medicine in the First Year of Life. J Nucl Med 2011; 52(6):905-925. Rationales A. Is incorrect since there is a significant difference in the volume of material injected into the patient. Clearly and 99mTc-MDP solution has a much smaller volume that the CT and MRI contrast agents. B. Is incorrect as the volume of injected 99mTc-MDP solution is much lower than the other two agents. C. Correct answer D. Incorrect answer. The masses among the three agents are vastly different. The mass of 99mTc-MDP is orders of magnitude lower than those of CT and MRI contrast agents. E. Incorrect answer. The mass of administered 99mTc-MDP is not greater than the masses of CT and MRI contrast agents. 2. Administration of radiopharmaceuticals in children results in which of the following? A. No pharmacologic effect B. Hemodynamic effect C. Hyperosmotic effect D. Toxic effect E. Frequent allergic reactions Correct Answer: A References 1. Treves ST, Baker A, Fahey FH, Cao X, Davis RT, Drubach LA, Grant FD, Zukotynski K. Nuclear Medicine in the First Year of Life. J Nucl Med 2011; 52(6):905-925. 2. Grant, FD. Thyroid. In Pediatric Nuclear Medicine and Molecular Imaging, 4th Edition. New York: Springer, 2007 Rationales A. Correct answer. Radiopharmaceuticals are given in trace amounts that do not produce a pharmacologic effect. B. Incorrect. The volume of injected tracer is very low (usualy <0.5 mL) and will not trigger a hemodynamic effect. C. Incorrect. No hyperosmotic effect is triggered by the intravenous administration of radiopharmaceuticals. D. Incorrect. There are no obvious toxic effects following the administration of radiopharmaceuticals. E. The amount of mass injected in very tiny and is below the threshold necessary to trigger and allergic reaction. For example, patients that are known to be allergic to iodine can be safely injected with radiopharmaceuticals containing iodine such as iodine -123 or iodine131. Bone Scintigraphy-State of the Art Helen R. Nadel, MD 3. Tc-99m MDP SPECT-CT -bone imaging in children is proving most helpful in the diagnosis of? A. Metastatic neuroblastoma. B. Occult bone injury in nonverbal children. C. Chronic regional pain syndrome. D. Chronic recurrent nonbacterial osteomyelitis. Correct Answer: B References 1. Nadel HR Pediatric bone scintigraphy update Semin Nucl Med. 2010 Jan; 40(1):31-40. 2. Van der Wall H, et al. Radionuclide bone scintigraphy in sports injuries. Semin Nucl Med 2010; 40:16–3 Shammas A. Nuclear medicine imaging of the pediatric musculoskeletal system. Semin Musculoskelet Radiol. 2009 Sep;13(3):159-80. Review. 3. Scharf S. SPECT/CT imaging in general orthopedic practice. Semin Nucl Med.2009 Sep;39(5):293-307. Review. 4. Nadel HR. SPECT/CT in pediatric patient management. Eur J Nucl Med Mol Imaging. 2014 Feb 20. [Epub ahead of print] PubMed PMID: 24554052. Rationales B is the correct answer. MDP bone scintigraphy can localize with sensitivity bony abnormality but SPECT/CT will improve specificity for diagnosis of occult fracture or myositis ossificans in nonverbal or handicapped children in whom localization of pain is not always clinically possible. A, C, and D. Bone scintigraphy may be abnormal in the other diagnoses but SPECT/CT will not increase the specificity of diagnosis in the other diagnoses listed. 4. Which of the following is true regarding the use of F-18 PET bone scans in children and young adults? A. F-18 PET requires anatomic correlation with diagnostic CT for evaluation of sports injuries. B. F-18 PET has a much higher radiation dose than 99mTc-MDP SPECT. C. F-18 PET is useful to assess skeletal metastases, but not benign bone disease. D. F-18 PET provides faster patient throughput than 99mTc-MDP SPECT. Correct Answer: D References 1. Grant FD, Fahey FH, Packard AB, Davis RT, Alavi A, Treves ST. Skeletal PET with 18F-fluoride: applying new technology to an old tracer. J Nucl Med 2008;49:68-78. Rationales A is incorrect – diagnostic CT is not required for identification of pars stress injury in the spine or stress injuries of the extremities. B is incorrect – The effective dose of F-18 PET is similar or minimally higher than the effective dose of 99mTc-MDP SPECT. C is incorrect – F-18 PET is particularly useful for the assessment of benign bone processes. D is the correct answer. The short uptake period (30-60 minutes) for F-18 PET bone scans shortens the overall time from dose administration to completion of scan. Pediatric Diuresis Renography Massoud Majd, MD, FACR 8-month-old male with left hydronephrosis. 5. Diuresis Renogram in an 8-month-old boy with prenatal diagnosis of left hydronephrosis demonstrates normal function, and a postdiuresis drainage halftime of 40 minutes. Which of the following statements best describes your interpretation of the study and the next step recommendation for T1/2 = 40 min this patient? A. The study is finished. The washout half-time of 40 minutes is diagnostic of high ET 020501514 grade ureteropelvic junction (UPJ) obstruction and you refer the patient to Urology for pyeloplasty. B. The study is finished. There is high probability for UPJ obstruction and you recommend a follow-up diuresis renogram in 6 months time to reassess drainage. C. You are concerned about UPJ obstruction and you ask the technologist to obtain a 3hour delayed image. D. You consider the study unfinished and ask the technologist to obtain static images before and after the patient is kept in upright position for 15 minutes to assess gravityassisted drainage, prior to final interpretation of the scan. Correct Answer: D References 1. Majd M. Nuclear Medicine in Pediatric Nephrology and Urology. Chapter in Diagnostic Nuclear Medicine, 4th Edition. Sandler MP et al, Editors. Lippincott Williams and Wilkins. Philadelphia. 2003, p. 1083-1106. 2. Wong DC, Rossleigh MA, Farnsworth RH. Diuretic renography with the addition of quantitative gravity-assisted drainage in infants and children. J Nucl Med 2000;41:103-1036. Rationales A. This is an incorrect answer because although post-diuresis drainage half-time is an important parameter in quantitative analysis of diuresis renogram curve, it should not be used in isolation. Poor drainage in supine may be positional and may improve after upright positioning. In addition, the natural history of neonatal hydronephrosis is variable and most of the time, the definitive diagnosis cannot be made on just the initial study, as the drainage may change over time. Therefore, poor post-diuresis drainage in supine position as seen in this infant should not be interpreted as definite evidence of obstruction and an indication for pyeloplasty. Quantitative evaluation of post-upright clearance of the high residual tracer activity at the end of 30 minutes imaging is very important in planning the follow-up imaging evaluation and the patient’s management. Poor drainage in upright position usually increases the likelihood of gradual worsening of obstruction, while in most cases with markedly improved drainage in upright position the follow-up studies show improved hydronephrosis and post-diuresis drainage as demonstrated by the examples demonstrated in the Figures 2,3,4,and 5. Answer b is also incorrect. Although a post-diuresis drainage half-time of 40 minutes is worrisome for UPJ obstruction and certainly indicates the need for follow-up imaging studies such as renal sonography and/or diuresis renography, this initial study should not be considered as complete without evaluating gravity-assisted drainage as described in the explanation given for answer a. Answer c is also incorrect. The post-diuresis drainage in the supine position is prolonged and there is certainly concern for UPJ obstruction. However, a delayed image will merely give you a visual inspection of further drainage from the collecting system without the ability to do a quantitative analysis of the drainage. Furthermore, standardization of the technique of gravityassisted drainage (10 minutes or 15 minutes of upright positioning) is important in comparing multiple studies in the same patient to assess for improvement or worsening of drainage on the follow-up exams. D. This is the correct answer. Patient’s supine position during diuresis renography can affect the post-diuresis drainage of a the tracer from the dilated system. It has been shown that the presence or lack of significant improvement of drainage after upright positioning is helpful in distinguishing obstructed from non-obstructed systems. This may affect management of the patient as demonstrated in the initial and follow-up diuresis renogram curves of two infants with prolonged post-diuresis washout half-times, one with good post-upright drainage (Figures 2 and 3) and one with poor post-upright drainage (Figures 4, 5 and 6). Case 1 Post-upright 65% clearance ET 020501514 Fig 2. Initial study at 8 months of age. The post-upright clearance in this patient with a washout halftime 40 minutes was 65%. Follow-up Case 1 at 20 mos of age T1/2 = 6 min ET 020501514 Fig 3. Follow-up study at 20 months of age showed markedly improved post-diuresis drainage with a washout half-time of 6 minutes. Case 2—Initial study T1/2 = 27 min Post-upright 4% clearance 020673350 Fig 4. The initial study in another infant at 4 months of age demonstrated a washout half-time of 27 minutes and a post-upright drainage of only 4%. Follow-up Case 2 at 7 mos of age 020673350 Fig 5. The followup study at 7 months of age showed marked worsening of the post-diuresis washout half-time (flat time-activity curve). Patient underwent pyeloplasty. Initial study at 3 months of age with 4% clearance in upright position Follow-up study at 7 months of age T1/2 = 27 min Post-pyeloplasty Fig 6. Diuresis renogram curves before ad after pyeloplsty in the infant with prolonged washout halftime and only 4% drainage in upright position. 5-YEAR-OLD BOY WITH INTERMITTENT ABDOMINAL PAIN 6. A 5-year-old boy with intermittent abdominal pain and sonographic diagnosis of mild left hydronephrosis underwent diuresis renography 6 weeks after an episode of pain to rule out left UPJ obstruction. The study demonstrated normal left renal function with a post-diuresis washout halftime of 9 minutes and 11% T1/2 = 9 min residual at 30 minutes. Residual at 30 min = 11% Which of the following statements best describes your interpretation of the study and the next step recommendation for this patient? 8/15/2011 020924176 A. The study is normal. UPJ obstruction is ruled out as the cause of abdominal pain. GI evaluation is recommended. B. The study is normal. But intermittent UPJ obstruction cannot be excluded. Repeat diuresis renography during or within 24 hours of pain episode is recommended. C. The study is normal. But intermittent UPJ obstruction cannot be excluded. Repeat diuresis renography 1-2 weeks after abdominal pain episode is recommended. Correct Answer: B References 1. Sparks et al. Evaluation of differential function and renographic patterns in patients with Dietl’s crisis. J Urol 2012;189(2):684-689. 2. Belman AB. Ureteropelvic junction obstruction as a cause for intermittent abdominal pain in children. Pediatrics 1991;88:1066-1069. Rationales a is incorrect answer. The post-diuresis drainage seen in this study can be interpreted as normal (no evidence of UPJ obstruction) in a 5-year-old child with hydronephrosis who is asymptomatic. But it does not exclude intermittent UPJ obstruction in patients with history of intermittent episodes of abdominal pain particularly when the pain is associated with nausea/vomiting (Dietl’s crisis). b is the correct answer. Dietl’s crises in children and adolescents with known or unknown hydronephrosis are due to episodes of transient acute UPJ obstruction of varying severity and duration. Acute obstruction causes decreased renal perfusion and severe decrease in the glomerular filtration rate (GFR). While the acute obstruction and pain symptoms are transient, the recovery of the GFR is gradual and may take a week to return to normal. MAG-3 is a tubular agent but its clearance from the cortex is dependent on glomerular filtration and urine flow through the tubules. Therefore, the renal scan and diuresis renogram findings vary depending on when the study is done in relation to the pain episode. If the study is done during or shortly after an episode of pain, the MAG 3 renal scan will often show decreased uptake but with complete or severe cortical retention of the tracer as seen on the renal scan done in this patient while he was in pain (Fig 7). If the study is done within a few days after the transient obstruction, it may show better renal function and good post-diuresis clearance of the tracer from the renal pelvis, but with varying degrees of cortical retention. Unilateral cortical retention of MAG3 in patients with intermittent abdominal pain is pathognomonic of ongoing or recent acute obstruction and a clear indication for pyeloplasty. c is incorrect answer because GFR eventually returns to normal level resulting in normal cortical clearance of the tracer and most likely no evidence of obstruction. Fig 8. MAG3 renal scan of the same patient who had a normal diuresis renogram 2 days before. This study was done when the patient had flank. It shows complete cortical retention of MAG3 in the left hydronephritic kidney and no evidence of tracer accumulation in the renal pelvis. The study is finished. Furosemide should not be injected. While he had left flank pain (8/17/2011) 020924176 Pediatric Gastrointestinal Scintigraphy Stephanie Spottswood, MD, MSPH 7. You are shown early and delayed images from a neonatal hepatobiliary imaging study. Which one of the following statements is true regarding hepatobiliary imaging in a neonate with elevated conjugated hyperbilirubinemia? A. Neonatal hepatitis and biliary atresia have distinctly different clinical, biochemical and histologic features B. Sensitivity and specificity for diagnosis of extrahepatic biliary atresia is approximately 52% and 44%, respectively C. Biliary atresia is excluded if the radiopharmaceutical progresses into the small bowel D. Pretreatment with phenobarbital for 5 days prior to imaging is not useful in distinguishing biliary atresia from other causes of neonatal cholestasis Correct Answer: C References 1. Landing BH. Considerations of the pathogenesis of neonatal hepatitis, biliary atresia and choldedochal cyst – the concept of infantile obstructive cholangiopathy. Prog Ped Surg 1974; 6:113-139 2. Kwatra N, Shalaby-Rana E, Narayanan S, Mohan P, Sunil G, Majd M. Phenobarbital-enhanced hepatobiliary scintigraphy in the diagnosis of biliary atresia: two decades of experience at a tertiary center. Pediatr Radiol 2013; 43: 1365-1375 3. Majd M, Reba RC, Altman RP: Effect of phenobarbital on 99mTc-IDA scintigraphy in the evaluation of neonatal jaundice. Semin Nucl Med 1981; Vol XI (3):194-204 4. Nadel HR. Hepatobiliary scintigraphy in children. Semin Nucl Med 1996; 26(1):25-42 Rationales A. is not correct. Hepatitis and biliary atresia have similar clinical presentations, as well as similar biochemical and histologic features. It has been hypothesized that neonatal hepatitis, biliary atresia and choledochal cyst represent variable outcomes of a single process termed: “infantile obstructive cholangiopathy”. Hepatobiliary imaging is the most reliable non-surgical means of distinguishing the two entities. B. Is not correct. The sensitivity and specificity for diagnosis of biliary atresia are much higher. In a recent study of 186 infants by Kwatra et al, sensitivity, specificity, and accuracy were 100%, 93%, and 94.6%, respectively, in children who underwent phenobarbital-enhanced hepatobiliary scintigraphy. C. Is correct. Biliary atresia can be reliably excluded with hepatobiliary imaging when there is passage of the radiopharmaceutical from the biliary system into the small bowel. D. Is not correct. Pretreatment with phenobarbital (5mg/kg/day) for 5 days prior to imaging is recommended to optimize hepatic uptake and excretion of the radiopharmaceutical. A serum phenobarbital level of 15 mcg/ml should be achieved prior to imaging. Ventilation/Perfusion Scans Lisa J. States, MD 8. A perfusion scan shows uptake in the brain, kidneys and thyroid. Choose the single best answer A. Free Technetium B. Left to Right shunt C. Right to Left shunt D. Metastatic neuroblastoma E. Chronic lung disease Correct Answer: C Reference 1. Grant FD, Treves ST . Nuclear Medicine and Molecular Imaging of the Pediatric Chest: Current Practical Imaging Assessment. Radiol Clin N Am 49 (2011) 1025-1051 NM Evaluation of CSF Shunts Hedieh K. Eslamy, MD 9. Images from a NM shuntogram performed in a patient with shunted hydrocephalus and a ventriculoperitoneal shunt are shown. What is the MOST LIKELY diagnosis? A. Occlusion of the proximal catheter B. Occlusion of the distal catheter C. Fracture of the distal catheter D. Extravasation of radiotracer at injection E. Valve malfunction Correct Answer: D References 1. Beril Gok, Sachin Batra, Hedieh Eslamy, Daniele Rigamonti, and Harvey Ziessman. Radionuclide Shunt Patency Study for Suspected Ventriculoatrial Shunt Malfunction. Clin Nucl Med. 2013;38: 527533. 2. Vernet O, Farmer JP, Lambert R, Montes JL. Radionuclide shuntogram: adjunct to manage hydrocephalic patients. J Nucl Med. 1996;37(3):406-410. 10. Lymphoscintigraphy cannot be performed with which radiotracer? A. 99m Tc-antimony trisulfide colloid. B. 99m Tc-dextran C. 99m Tc-sulfur colloid D. 99m Tc-serum albumin Correct Answer: C (Has to be triple filtered.) References 1. Zinwmeister MS Lymphoscintigraphy: Current techniques and indications 26: No 7, 1997. Oncologic Imaging Michael J. Gelfand, MD and Susan E. Sharp, MD 11. In regard to [F-18]FDG PET/CT imaging in lymphoma: A. Imaging of the lower extremities may be omitted on follow-up studies, if the lower extremities were normal on the initial PET/CT study at presentation prior to therapy. B. FDG PET/CT imaging in lymphoma is often falsely negative when residual masses remain after chemotherapy. C. At early follow-up, after one or two cycles of chemotherapy, FDGPET/CT imaging in lymphoma is predictive of outcome. D. Measurements of standardized uptake value (SUV) are routinely used to evaluate response to therapy. E. A and C. Correct Answer: E References 1. Sammer MB, Shulkin BL, Alessio A, Parisi MT. Role of limited whole-body PET/CT in pediatric lymphoma. AJR Am J Roentgenol. 2011 May;196(5):1047-55. 2. Kostakoglu L, Coleman M, Leonard JP, Kuji I, Zoe H, Goldsmith SJ. PET predicts prognosis after 1 cycle of chemotherapy in aggressive lymphoma and Hodgkin's disease. J Nucl Med. 2002 Aug;43(8):1018-27. 3. Miller E, Metser U, Avrahami G, Dvir R, Valdman D, Sira LB, Sayar D, Burstein Y, Toren A, Yaniv I, Even-Sapir E. Role of 18F-FDG PET/CT in staging and follow-up of lymphoma in pediatric and young adult patients. J Comput Assist Tomogr. 2006 Jul-Aug;30(4):689-94. 12. What is the first line functional imaging agent used in neuroblastoma? A. F-18-FDG B. I-131-MIBG C. I-123-MIBG D. Tc-99m-MDP E. In-111-Octreotide Correct Answer: C Rationales I-123-MIBG is the first line functional imaging agent used in neuroblastoma due to its high sensitivity and specificity for disease detection. I-123-MIBG is preferred over I-131-MIBG as it gives higher quality images at a lower radiation dose. Use of F-18-FDG for neuroblastoma imaging is increasing, especially in patients with non-MIBG avid disease. Tc-99m-MDP bone scans may be used to assess cortical bone metastases at diagnosis, but provide little or no additional information during follow-up of patients with MIBG-avid disease. In-111-Octreotide is not commonly used for neuroblastoma imaging. References 1. Monclair T, Brodeur GM, Ambros PF, et al. The International Neuroblastoma Risk Group (INRG) staging system: an INRG task force report. J Clin Oncol 2009;27(2):298-303. 2. Brisse HJ, McCarville MB, Granata C, et al. Guidelines for imaging and staging of neuroblastic tumors: consensus report from the International Neuroblastoma Risk Group Project. Radiology 2011;261(1):243-57 3. Sharp SE, Gelfand MJ, and Shulkin BL. Neuroblastoma: Functional Imaging. In: Treves ST, ed. Pediatric Nuclear Medicine and Molecular Imaging. Fourth Edition. New York, NY: Springer SBM; 2014: Chapter 19. NM Infection Imaging in Children Marguerite T. Parisi, MD, MS Ed 13. Advantages of F-18 FDG PET or PET/CT in the evaluation of infection include all of the following EXCEPT: A. Delayed normalization of FDG-uptake in post-traumatic or post-surgical sites. B. High spacial and contrast resolution C. High sensitivity for chronic infections D. Ability to quickly obtain results compared to gallium or radio-labelled white cell scans Correct Answer: A Rationales Correct answer is A. As opposed to the radionuclide bone scan, FDG uptake rapidly normalizes following traumatic or surgical fractures as fibroblasts predominate during normal healing. More over FDG accumulation quickly subsides within 3-4 months following surgery. Choices B-D are all advantages of FDG-PET or PET/CT compared to the other radiotracers used for evaluation of infections 14. All of the following regarding the role of F-18 FDG PET or PET/CT in musculoskeletal infections are true EXCEPT: A. Highly sensitive for diagnosis of acute and subacute bone and soft tissue infections. B. Not adversely affected by the presence of metallic hardware. C. Cannot reliably distinguish infection from non-infectious inflammation or malignancy D. Imaging procedure of choice for diagnosis of uncomplicated osteomyelitis. Correct Answer: D Rationales Correct answer is D. F-18 FDG PET or PET/CT is of limited value in diagnosing uncomplicated osteomyelitis compared with the combination of physical examination, evaluation of biochemical marker alteration, and 3-phase bone scan (Tc-99m MDP). This is particularly true in children given the frequent need for sedation and higher patient radiation dose of F-18 FDG compared to Tc 99m MDP bone scan. Choices A-C are all true regarding the role of FDG-PET or PET/CT in children and adults with musculoskeletal infections. References 1. Stumpke KD, et al. Infection imaging using whole-body FDG-PET. Eur J. Nucl Med 2000:27:822-832 2. Basu S, et al. Positron emission tomography as a diagnostic tool in infection: present role and future possibilities. Semin Nucl Med 2009; 391:36-51. 3. Parisi, MT. Functional Imaging of Infection: Conventional nuclear medicine agents and the expanding role of 18-F FDG/PET; an overview. Pediatr Radiol 2011; 41: 805-810. 4. Servaes S. Imaging Infection and Inflammation in Children with 18-F FDG PET and 18-F-FDG PET/CT. J Nucl Med Technol 2011; 39:179-182. 15. The most common presentation for ischemic stroke in newborn infants is: A. increased irritability, inconsolability B. headache and confusion C. seizures D. focal neurologic deficit e.g. hemiparesis E. all of the above Correct Answer: C Rationale The correct answer is c). Seizures alone are characteristic of neonates with arterial or venous ischemic stroke. The neonatal brain is immature and is less likely to show a focal deficit e.g. hemiparesis than older infants and children. References 1. Nelson KB, Lynch JK. Stroke in newborn infants. Lancet Neurol. 2004;3:150 –158.42. 2. deVeber G, Andrew M, Adams C, et al. Cerebral sinovenous thrombosis in children. N Engl J Med. 2001; 345:417– 423. FDG PET: Neurologic Applications A. Luana Stanescu, MD 16. Normal FDG PET brain uptake pattern can show hypermetabolism in all of the following brain areas except: A. Basal ganglia B. Frontal eye fields C. Posterior cingulate gyrus D. Frontal and parietal association cortex in infants E. Wernicke areas Correct Answer: D Rationale Options A, B, C and E: Incorrect. The basal ganglia normally demonstrate hypermetabolism compared with the white matter on FDG PET images. More focal hypermetabolism has also been described in certain cortical areas, such as the posterior cingulate gyrus, the Wernicke region, and the frontal eye fields. Option D; Correct. The brain glucose metabolic pattern in infants reflects the functional brain maturation, with the frontal and parietal association cortex demonstrating lower FDG uptake, in a pattern similar to that in patients with Alzheimer disease, and progressively increasing until 1 year of age, when the pattern becomes similar to that in adults. References 1. Mettler FA Jr, Guiberteau MJ. Essentials of nuclear medicine imaging. 5th ed. Philadelphia, Pa: Saunders Elsevier, 2005; 379, 388–393. 2. Chugani HT, Phelps ME. Imaging human brain development with positron emission tomography. J Nucl Med 1991;32(1):23–26. PET/MR: Implementing a Clinical Program Victor Seghers, MD, PhD 17. Which of the following is true regarding current MR Attenuation Correction algorithms used in PET/MR? A. Not yet FDA-approved B. Currently only validated for Brain PET/MR C. Does not Differentiate Bone from Soft Tissue D. Create fewer artifacts relative to CT Attenuation Correction E. Still utilizes ionizing radiation Correct Answer: C Rationale Option A is NOT correct: The current MR Attenuation Correction Algorithms were FDA approved in 2010. Option B is Not correct: PET/MR is clinically validated by the FDA for use without restriction to body part. Option C is CORRECT: The current commercially available attenuation corrections methods include: Philips three segment (air, soft tissue, and lungs) and Siemens four segment (air, soft tissue, fat, and lungs). Bone is not differentiated from soft tissue in either of these 2 methods which may lead to quantitative errors compared to CT-based attenuation correction methods. Option D is NOT correct: Both CTAC and MRAC methods can cause imaging artifacts. Option E is NOT correct: MRAC does not utilize ionizing radiation. References 1. Image quality assessment of automatic three-segment MR attenuation correction vs CT attenuation correction; Partovi S et al; Am J Nucl Med Mol Imaging 2013;3(3):291-299