Case Report
advertisement

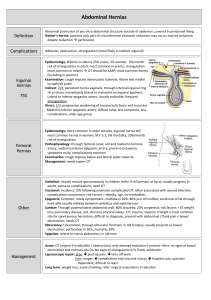
Introduction : A hernia is the protrusion of viscus through an abnormal opening in the walls of its containing cavity. An indirect inguinal hernia is still the most common cause of hernias in females following incisional hernias1. Indirect inguinal hernia in females is 4 % as common as in males with an overall incidence of 1-2% in females2. It is almost always congenital and presents usually in childhood3. Case Report : Our patient, 35 years, female, Para5 Living5, residing at Panvel, belonging to a middle socio-economic strata came to our opd with complains of swelling and itching at the vulva since 10 days. Patient had no other complains and no significant past history. She was married since 17 yrs with history of tubal ligation done 2 yrs back. She had 5 Full term normal deliveries with last child birth 2 yrs back and weighed 54.36 kgs with a BMI of 21.23kg/m2. On local examination, a swelling was seen on the right labia. Skin over the swelling was normal with no signs of fistulas or sinuses or dilated veins. It was non tender, no redness or raised temperature, not easily reducible, transillumination was negative and swelling decreased on lying down with a positive cough impulse. On Palpation gurgling was felt (peristalsis) s/o bowel. A differential diagnosis was made of indirect inguinal hernia or encysted hydrocele of canal of Nuck. Surgery opinion was taken and diagnosis was confirmed as an indirect inguinal hernia. Patient underwent a right sided Lichenstein hernioplasty under spinal anaesthesia. Intra-operatively round ligament and the right ovary was found to be part of the contents of the hernia sac and were reposited. There were no signs of incarceration or strangulation of bowel and no evidence of torsion of the ovary. The posterior wall was reinforced with a polypropelene mesh. Patient was managed post operatively on antibiotics and analgesics. Patient was discharged on Day 5 post operatively with no complains. Discussion : Indirect Inguinal Hernia is the most common cause of hernia in females with the overall risk of 1-2% of a female to develop a hernia in her lifetime. The hernial sac may contain bowel, omentum, the appendix and any pelvic organ such as the ovary, fallopian tube and in a few reported cases of congenital hernias even the uterus4. In such cases there may also be associated Mullerian Duct anomaly such as a unicornuate uterus4. The hernial sac is lined by the round ligament in females5. Inguinal Hernias in women are always indirect and direct inguinal hernias almost never occur in females. It is almost always congenital and presents usually in childhood before five years of age3. In case of congenital hernias we need to rule out intersex syndromes especially in cases of bilateral inguinal hernias which is usually associate with complete androgen insensitivity syndrome (CAIS)6. The inguinal canal widens with age. Thus in females, an indirect inguinal hernia usually occurs in two age groups; the paedatric and the geriatric. There are a few predisposing factors in women:1. 2. 3. 4. 5. 6. 7. Pregnancy Smoking because of the acquired collagen deficiency it causes Multi parity Chronic cough/constipation Lifting heavy weights Heavy strenuous exercise as in athletes and labourers Obesity : Although obesity used to be considered as a predisposing factor for hernias both in males as well as females with the theory that it causes abdominal muscle weakness, a few studies have shown little or no difference in the incidence of hernias with only obesity as the risk factor7 Nyhus described a spectrum of hernias differentiated by size, presence or absence of a sac, and the degree of deformity of anatomy. Type III hernias are more common in men, whereas Type I and II hernias (occult hernias) appear to be more common in women8. Our case was unique as this was a type III hernia which occurred in a female of a reproductive age group with no other complains besides a genital swelling. In adult females the most common complain is that of a groin mass. The second most common complain is that of chronic pelvic pain or groin pain or ovarian pain as described by patients9,10. The patient may even complain of dyspareunia. Pain usually occurs in the incipient phase of hernia due to the stretching of the tissues. The pain maybe a sharp, shooting pain similar to neuralgias and may even be associated with back pains or sciatica10. In case of small hernias associated with pain, the patient can be managed on analgesics and anti-inflammatory drugs and physiotherapy. In large hernias or with signs of obstruction or strangulation, the management is surgical. Surgery maybe an open surgery such as Lichenstein’s hernioplasty with a mesh or today more popularly it is done laparoscopically. However during surgery, it is crucial to explore the other spaces of the abdomen such as the femoral and obturator canals thoroughly because such women may have other associated occult hernias as well11. Conclusion : Indirect inguinal hernia in adult women of reproductive age group is a rarity in itself and it can be easily misdiagnosed. A large swelling can be mistaken for a cyst or a hydrocele. A small swelling may go unnoticed. Most gynecologists and general surgeons are unaware of occult hernias and many do not believe that they exist; and therefore, they are controversial9. Albeit rare, inguinal hernia must be kept in mind when diagnosing a patient with a groin swelling or chronic pelvic pain especially in high risk women. References 1. Inguinal Hernia in Female Infants and Children RICHARD GOLDSTEIN, M.D., WILLIS J. POrrS, M.D., Department of Surgery of the Children's Memorial Hospital, Chicago, Illinois 2. John T Jenkins, Patrick J O’Dwyer (2008). "Inguinal hernias". BMJ 336 (7638): 269–272 3. Chen-Sheng Huang, Chih-Cheng Luo, European Journal of Pediatrics, July 2003, Volume 162, Issue 7-8, pp 493-495, The presentation of asymptomatic palpable movable mass in female inguinal hernia 4. David C. Elliott, MD; Thomas E. Beam, MD; Thomas S. Denapoli, MD, Hernia Uterus Inguinale Associated With Unicornuate Uterus, Arch Surg. 1989;124(7):872-873 5. Ando, H., Kaneko, K., Ito, F., Seo, T. and Ito, T. (1997), Anatomy of the round ligament in female infants and children with an inguinal hernia. Br J Surg, 84: 404–405. 6. ASMA DEEB and IEUAN A. HUGHES,University Department of Paediatrics, Cambridge University, Cambridge, UK,30 March 2005 7. Mike S. L. Liem, Yolanda van der Graaf, Reinder C. Zwart, Risk Factors for Inguinal Hernia in Women: A Case-Control Study, Am J Epidemiol Vol. 146, No. 9, 1997 8. Nyhus LM. Individualization of hernia repair: a new era. Surgery. 1993;114:1-2. 9. DEBORAH A. METZGER, PhD, MD, HERNIAS IN WOMEN: UNCOMMON OR UNRECOGNIZED?, January 01, 2004, Laparoscopy today 10. Kavic MS. Chronic pelvic pain, hernias and the general surgeon [editorial].JSLS. 1999;3:89-90. 11. Metzger DA, Daoud I. Occult hernias in women with chronic pelvic pain. Plenary abstract presented at: International Congress of Gynecologic Endoscopy, American Association of Gynecologic Laparoscopists 26th Annual Meeting; September 24-28, 1997, Seattle, WA.