letter to the editor

Anesth Analg 2006;103:1620-1621
© 2006 International Anesthesia Research Society doi: 10.1213/01.ane.0000246433.84413.49
LETTER TO THE EDITOR
Editor-in-Chief Steven L. Shafer
Recovering a Detached Univent Endobronchial Balloon
Abdullah M. Kaki, FRCPC, FRCPC, and Essam E. Abd El-Hakeem, MD
Department of Anesthesia; Faculty of Medicine; King Abdul Aziz University Hospital; Jeddah, Saudi Arabia; amkaki@yahoo.com
To the Editor:
The Univent ® endotracheal tube from Fuji Systems Corporation, To kyo, Japan has a movable endobronchial blocker used for one-lung ventilation. We report a potentially serious complication with the Univent endobronchial tube that occurred during thoracoscopic surgery in a pediatric patient.
A 3-yr-old, 14.5-kg, 84-cm girl underwent right-sided thoracoscopy.
After inducing general anesthesia, we successfully isolated the right lung, using a size 3.5 Univent endobronchial tube with an inflated balloon. We positioned the patient, inflated the blocker, and re-inserted the bronchoscope to confirm position.
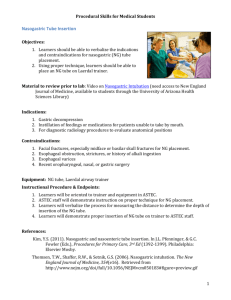
We found that the endobronchial balloon was completely detached, lying in the right mainstem bronchus. We were unable to remove the balloon with the suction port on the flexible bronchoscope, but eventually removed it using a suction catheter attached to the proximal end of the Univent endotracheal tube after the advancement of the tube nearer to the balloon ( Fig. 1 ). We re-intubated the trachea with another size 3.5 Univent tube, and the rest of operation was uneventful.
Figure 1.
The removed Univent tube. The detached distal balloon lies within the circle
View larger version (127K):
[in this window]
[in a new window]
Anesth Analg 2006;103:1062
© 2006 International Anesthesia Research Society doi: 10.1213/01.ane.0000239063.48453.9f
LETTER TO THE EDITOR
Editor-in-Chief Steven L. Shafer
A Simple Technique to Avoid Traumatic Nasal Intubation
Abdullah M. Kaki, MD, FRCPC, and Walid A. Alyafi, MD, FRCPC
Department of Anesthesia; Faculty of Medicine; King Abdalaziz Unversity Hospital; amkaki@yahoo.com
(Kaki)
Department of Critical Care; King Abdalaziz National Guard Medical City; Jeddah, Saudi Arabia (Alyafi)
To the Editor:
Nasotracheal intubation is the preferred method to control the airway for several types of surgery.
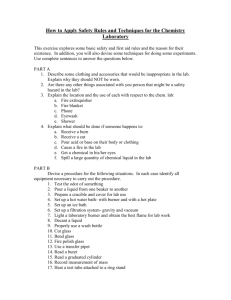
Many techniques have been prescribed to reduce nasal mucosa damage. We have been using a nasogastric tube as an internal stylet to facilitate threading the nasotracheal tube. Before intubation, we cut the proximal suction port of nasogastric tube, and lubricate it with watersoluble jelly. ( Fig. 1 ) Then we introduce the nasogastric tube into the largest patent nares and thread it gently into the posterior pharynx. We then thread the nasotracheal tube through the nostril and into the pharynx over the nasogastric tube. The nasogastric tube is then removed, and we use a Magill forceps to direct the nasotra-cheal tube into the trachea. We have used this method in 10 children and 15 adults, with little trauma and bleeding.
View larger version (107K):
[in this window]
[in a new window]
Figure 1.
Endotracheal tube is threaded on the nasogastric tube and in the middle the suction port is cut.