Cutting Down on Colstridium Difficile

Running Head: CUTTING DOWN ON CLOSTRIDIUM DIFFICILE 1
Cutting Down on Clostridium Difficile
Point of Contact: Scott Reynolds, Infection Control Specialist
James H. Quillen VA Medical Center, P.O. Box 4000, Mountain Home, TN 37684
(423)926-1171 X7542, Scott.Reynolds@va.gov
Group Involved with the Project: Infection Control Department, along with
Environmental Management Service, Nursing Service, Clinical Providers and Staff
Submitted by Tara K. Egbert
10 May 2013
Executive Summary: Current evidence based practice indicates a bundled approach to control
Clostridium difficile infection rates similar to the approach adopted by the Mountain Home VA
Medical Center in 2009. Mountain Home’s bundled strategy encompasses earlier contact isolation for patients with diarrhea, limiting use of broad spectrum antibiotics, optimizing environmental disinfection, daily surveillance, and staff education.
CUTTING DOWN ON CLOSTRIDIUM DIFFICILE 2
Objective of the Best Practice:
On Mountain Home VA Healthcare System’s quest to achieve top quality and efficiency rankings and be recognized as a healthcare leader relative to positive patient outcomes, the need to decrease the rate of Clostridium difficile infections in acute care was identified.
Background: Within the VHA, reducing healthcare associated complications of Clostridium difficile infection was identified as the focus for Fiscal Year 2011 by the Task Force chartered to further the Multi-drug Resistant Organisms Prevention Initiative (Department of Veterans
Affairs, 2012). Mountain Home identified the need to decrease Clostridium difficile infections in acute care as early as 2006, at which time, staff education and a hand washing campaign resulted in a decreasing trend in the rate of infection (Figure 1). Despite the positive strides; however, Mountain Home’s rate of infection still surpassed CDC benchmarks for top performing healthcare organizations (Mountain Home Healthcare System, 2012). It was clear to our leadership and clinical staff that more still needed to be done to achieve our facility goals for quality and improved patient outcomes. With the 2009 implementation of a multi-faceted approach to controlling Clostridium difficile, Mountain Home achieved a dramatic decrease in infection rates, bringing them well below the CDC benchmark. Continuous monitoring and staff re-education have helped the facility sustain this outcome. Mountain Home’s accomplishments in reducing the rate of Clostridium difficile infection distinguishes the organization from mainstream healthcare organizations who struggle to make similar strides. According to a 2013 survey done by the Association for Professionals in Infection Control and Epidemiology (APIC),
70% of respondents have adopted additional interventions to control Clostridium difficile infection rates since March 2010; however, only 42% of these facilities have seen any decline in infection rates (Pyrek, 2013).
Literature Review:
Commonly referred to by healthcare workers as “C. diff”, Clostridium difficile is an anaerobic, spore forming, gram positive rod; which means, in simple terms, these particular bacteria can survive without oxygen and are particularly difficult to eradicate.
According to Jennie Mayfield, BSN, MPH, CIC, President of the Association for Professionals in Infection Control and Epidemiology, and clinical epidemiologist states that new strains of
Clostridium difficile produce from 7 to 17 times more toxin than earlier strains of the bacteria causing more severe disease and higher mortality rates (Pyrek, 2013). Diarrhea associated with
Clostridium difficile is generally on the rise and Clostridium difficile is now the “most common cause of infectious gastrointestinal disease among hospitalized patients” (McMullen, Zack,
Coopersmith, Kollef, Dubberke, and Warren, 2007, p.205). Symptoms of C. diff infection range from moderate to severe watery diarrhea, mild to severe abdominal cramping, fever, loss of appetite, and nausea. Each year, 14,000 Americans die from healthcare associated Clostridium difficile infection (Pyrek, 2013). Hospitalization in and of itself increases a person’s risk for exposure to Clostridium difficile; however, more severely ill patients, older patients, and patients undergoing antibiotic therapy or gastrointestinal surgery are at even greater risk (McMullen et al,
2007). Compounding the problem is that the organism only responds to treatment with two drugs: metronidazole and vancomycin (Pyrek, 2013). The main vectors responsible for transmission of Clostridium difficile are colonized individuals, environmental surfaces, and contaminated equipment (McMullen et al, 2007).
CUTTING DOWN ON CLOSTRIDIUM DIFFICILE 3
Studies have evaluated several methods of environmental decontamination to reduce the spread of Clostridium difficile including the use of hypochlorite solution, the use of a hydrogen peroxide dry mist disinfection system, and the use of automated ultraviolet radiation.
Decontamination using hydrogen peroxide dry mist is time consuming and the literature is contradictory regarding its efficacy (Barbut, Menuet, Verachten, and Girou, 2009). In their study, McMullen et al. (2007) evaluated the efficacy of daily environmental cleaning with a hypochlorite solution in the entire MICU comparative to daily cleaning with the hypochlorite solution only in rooms occupied by patients with Clostridium difficile associated diarrhea in the
SICU . Both units showed a statistically significant decrease in rates of Clostridium difficile associated diarrhea. Interestingly, McMullen et al.’s study indicated no statistically significant difference in rates of infection with an earlier hand hygiene campaign in their study facility.
Implementation Methods: Following successes with “bundled strategies” to reduce central line associated bloodstream infections, ventilator associated pneumonia, and catheter associated urinary tract infections, Clostridium difficile infection prevention strategies using a similar
“bundled” approach are beginning to emerge (Segal, 2013). Led by the facility’s Infection
Control Specialist, Mountain Home was well ahead of the curve by implementing a multi-faceted approach to controlling Clostridium difficile infection rates as early as 2009. This approach, which continues to be implemented, entails “…earlier contact isolation for patients with diarrhea, limiting use of broad spectrum antibiotics, optimizing environmental disinfection, daily surveillance, and staff education” (Mountain Home Healthcare System, 2012, p.31). Mr. Scott
Reynolds, Infection Control Specialist stresses the importance of an interdisciplinary approach to staff education, routine re-education, and diligent teamwork to ensure that all elements of this prevention strategy are implemented consistently. All patients with known or suspected C. diff infection are placed on contact isolation and appropriate signage is placed on the patient’s door to alert clinical and Environmental Management Service staff that contact precautions are required. Environmental disinfection with a hypochlorite solution is done for all known or suspected cases of Clostridium difficile. Mountain Home’s bundled approach already in place meets the recent Department of Veterans Affairs 2012 mandate for all acute care facilities to implement a bundled approach including: 1.) environmental management, 2.) hand hygiene,
3.) contact precautions for symptomatic Clostridium difficile infection, and 4.) cultural transformation “where infection control becomes everyone’s business” (2012). Although
Mountain Home implemented a bundled strategy early on, current literature supports this evidence based practice. The University of Pittsburgh Medical Center reported a 71% reduction in Clostridium difficile infection rates from 2001 to 2006 with a similar bundled strategy including education, early case finding, expanded infection control measures, and antimicrobial management (Muto, Blank, Marsh, Vergis, O’Leary, Shutt, …and Paterson, 2007).
Results:
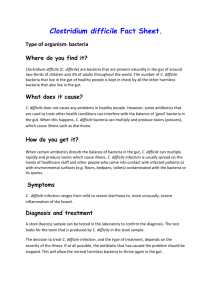
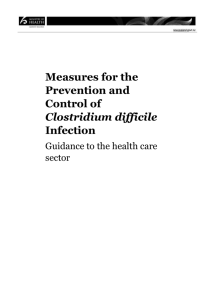
Mountain Home’s total number of patients positive for Clostridium difficile has shown a sustained downward trend since 2006 (Figure 1). Early efforts at controlling Clostridium difficile infection rates through staff education and a focused hand washing campaign did not begin to show positive results in acute care until 2008; however, implementation of the bundled strategy in 2009 resulted in a dramatic decrease in infection rates in 2010 (Figure 2). Although the staff education and hand washing campaign seemed to be more effective in extended care, additional gains were still achieved with the implementation of the bundled strategy (Figure 3).
CUTTING DOWN ON CLOSTRIDIUM DIFFICILE 4
Figure 1. Mountain Home Total Clostridium difficile Patients.
Mountain Home Clostridium difficile Healthcare Associated Rates
Acute Care
30
25.79
25
24.48
22.21
22.3
20
20.22
15
15.15
10
New C. diff reporting definitions instituted July
1,2012.
New C. diff test instituted
(Tox B PCR test) Sept. 29,
2012.
5
6.08
3.67
0
2005
2006
2007
2008
2009
2010
2011
2012
Year
Figure 2. Mountain Home Clostridium difficile Healthcare Associated Rates: Acute Care.
CUTTING DOWN ON CLOSTRIDIUM DIFFICILE
Mountain Home Clostridium difficile Healthcare Associated Rates
Extended Care
30
5
25
20
15
10
8
New C. diff reporting definitions instituted July
1, 2012.
New C. diff test instituted
(Tox B PCR test) Sept.
29, 2012.
6.49
5.88
5 5.21
4.4
3.13
1.34
0
0.68
2005
2006
2007
2008
2009
2010
2011
2012
Year
Figure 3. Mountain Home Clostridium difficile Healthcare Associated Rates: Extended Care.
Conclusion: While Mountain Home has made great strides in reducing the rate of Clostridium difficile infection, the infection control team is eager to add to their bundled strategy to further reduce infection rates. Although control measures typically focus on patients with Clostridium difficile associated diarrhea, at least one study suggests that further research needs to be conducted to determine the significance of the risk imposed by asymptomatic carriers of
Clostridium difficile particularly in long term care facilities (Riggs, Sethi, Zabarsky, Eckstein,
Jump, and Donskey, 2007). Riggs et al.’s study indicated that as much as 51% of asymptomatic patients were carriers of toxin producing Clostridium difficile. In fact, asymptomatic carriers outnumbered symptomatic patients 7 to 1 in their study sample. Previous infection with
Clostridium difficile (P<.001) and previous antibiotic use (P=.017) were statistically significantly associated with asymptomatic carriage; however, “the combination of these 2 variables was predictive of asymptomatic carriage” (2007, p992). Riggs et al. also identified length of hospitalization and frequency of antibiotic therapy as factors which contributed to risk of asymptomatic carriage of Clostridium difficile (2007). Riggs et al suggest 2 additional interventions to further decrease the rate of Clostridium difficile transmission: 1.) extend the duration of contact precautions beyond the resolution of diarrhea to the time of discharge and
2.) terminal cleaning with hypochlorite solution for all rooms when a patient is transferred or discharged (2007). Currently, there is no national practice recommendation relative to the duration of contact precautions (Pyrek 2013); however, Riggs et al.’s suggestion seems like a logical next step.
CUTTING DOWN ON CLOSTRIDIUM DIFFICILE
References
Barbut, F., Menuet, D., Verachten, M., and Girou, E. (2009). Comparison of the efficacy of a hydrogen peroxide Dry ‐ Mist disinfection system and sodium hypochlorite solution for
6 eradication of clostridium difficile spores. Infection Control and Hospital Epidemiology,
30 (6), 507-514. Retrieved from http://www.jstor.org/stable/10.1086/597232
Centers for Disease Control and Prevention (2013). Frequently Asked Questions about
Clostridium Difficile. Retrieved from http://www.cdc.gov
Department of Veterans Affairs (2012). Guideline for Prevention of Clostridium Difficile
Infection (CDI) in Veterans Health Administration Acute-Care Facilities.
McMullen, K.M., Zack, J., Coopersmith, C.M., Kollef, M., Dubberke, E., and Warren, D. K.
(2007). Use of hypochlorite solution to decrease rates of clostridium difficile–Associated diarrhea. Infection Control and Hospital Epidemiology, 28 (2), 205-207. Retrieved from http://www.jstor.org/stable/10.1086/511791
Mountain Home Healthcare System (2012). Robert W. Carey Award 2012 Application.
Muto, C. A., Blank, M. K., Marsh, J. W., Vergis, E. N., O'Leary, M. M., Shutt, K. A., Pasculle,
A.W., Pokrywka, M., Garcia, J. G., Posey, K., Robert, T. L., Potoski, B. A., Blank, G. E.,
Simmons, R. L., Veldkamp, P., Harrison, L. H., and Paterson, D. L. (2007). Control of an outbreak of infection with the hypervirulent clostridium difficile BI strain in a university hospital using a comprehensive "bundle" approach.
Clinical Infectious Diseases, 45 (10),
1266-1273. Retrieved from http://www.jstor.org/stable/4485692
CUTTING DOWN ON CLOSTRIDIUM DIFFICILE
Pyrek, K. M. (2013). New APIC Poll Reveals Ongoing Improvement Needed in Efforts to
7
Prevent and Control Clostridium Difficile. Infection Control Today : Clostridium Difficile:
Trends and Strategies for Prevention, April 2013, 1-10. Retrieved from www.infectioncontroltoday.com
Riggs, M. M., Sethi, A. K., Zabarsky, T. F., Eckstein, E. C., Jump, R. L. P., & Donskey, C. J.
(2007). Asymptomatic carriers are a potential source for transmission of epidemic and nonepidemic clostridium difficile strains among long-term care facility residents.
Clinical
Infectious Diseases, 45 (8), 992-998. Retrieved from http://www.jstor.org/stable/4485626
Segal, P. (2013). Strategies to Prevent Transmission of C. Difficile. Infection Control Today :
Clostridium Difficile: Trends and Strategies for Prevention, April 2013, 11-16. Retrieved from www.infectioncontroltoday.com
CUTTING DOWN ON CLOSTRIDIUM DIFFICILE
Appendix A
8
CUTTING DOWN ON CLOSTRIDIUM DIFFICILE 9