Greater Trochanter Pain Syndrome
advertisement

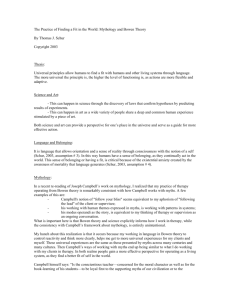
Diploma of Specialised Bowen Therapy 22006VIC Research Task – Traditional, Alternative and Scientific Practices in Medicine The Use of the Bowen Technique for Symptomatic Relief of Greater Trochanteric Pain Syndrome (GTPS) Michelle Mauro 2013 Diploma – Specialised Bowen Therapy Michelle Mauro Page 1 of 12 The Use of the Bowen Technique for Symptomatic Relief of Greater Trochanteric Pain Syndrome Introduction Many injuries and conditions, both acute and chronic have well established paths of treatment that follow western medical interventions; however these treatments may be costly, painful and invasive. The wider community, including medical practitioners, often have limited knowledge and information of complimentary, often less invasive, effective treatment alternatives. This research article will focus on Greater Trochanteric Pain Syndrome (GTPS) and aims to investigate the effectiveness of the Bowen Technique for the relief of symptoms associated with this painful condition. Evolution of Treatment and Greater Trochanteric Pain Syndrome Greater trochanteric pain syndrome is (GTPS) is a term used to describe chronic pain overlying the lateral aspect of the hip. Patients typically present with chronic, persistent pain in the lateral hip and/or buttock that is exacerbated by lying on the affected side, prolonged standing or transitioning to a standing position, sitting with the affected leg crossed, climbing stairs, running or other high impact activities (Williams & Cohen, 2009, p. 1665). The pain can radiate into the lower buttocks and the lateral aspect of the thigh, but rarely extends into the posterior aspect of the thigh or below the knee (Geraci et al, 2011, p. 76). The Greater Trochanter (GT) is the site of confluence of three main bursae, the hip abductor thigh muscles and the iliotibial tract. Histopathologic findings have shown GTPS results from both tendinopathy and bursa pathology arising from acute or repetitive trauma (Geraci et al, 2011, p. 75). Acute trauma includes contusions from falls, contact sports and other sources of impact. Repetitive trauma can include bursal irritation resulting from friction by the iliotibial band. This repetitive cumulative irritation often occurs in runners but can also be seen in less active individuals (Geraci et al, 2011, p. 76). The Greater Trochanter is the site of both tendinous insertions and bursa. The main tendon of the gluteus medius muscle attaches to the postero-superior aspect of the GT, with the lateral tendon inserting into the lateral aspect. The gluteus minimus muscle attaches to the anterior facet of the GT. Consequently, inflammation and tears of either the gluteus medius or minimus muscles, or their tendinous insertions, from tension imposed by the ITB and/or frictional trauma from overuse, may result in GTPS (Del Buona et al, 2011, p. ) Literature describes more than twenty bursae in the trochanteric area; however three are the most representative (Geraci et al, 2011, p. 75). The subgluteus minimus bursa; located between the gluteus minimus tendon and the anterior facet, the subgluteus medius bursa; lies deep to the portion of the lateral insetion of the gluteus medius tendon and the trochanteric Diploma – Specialised Bowen Therapy Michelle Mauro Page 2 of 12 bursa (or subgluteus maximus bursa); covers the posterior facet, lying deep to the gluteus maximus muscle extending laterally and distally (Klauser et al, 2013, p. 45). Overuse of the trochanteric bursa and or an inflammation of the bursa may cause trochanteric bursitis resulting in pain in the region of the greater trochanter (Geraci et al, 2011, p. 75). Figure 1. Anatomy of the trochanteric region. a = gluteus minimus muscle, b = gluteus medius muscle, c = subgluteus minimus bursa, d = subgluteus medius bursa, e = subgluteus maximus bursa, f = zona orbicularis of hip joint capsule, g = superior neck recess of hip joint, h = inferior neck recess of hip joint, i = vastus lateralis muscle, k = iliotibial band (Geraci et al, 2011, p. 75). Diploma – Specialised Bowen Therapy Michelle Mauro Page 3 of 12 Hip pain is present in all age groups but is more prevalent between the fourth and sixth decades of life (Williams & Cohen, 2009, p. 1663). GTPS is most frequent in women (F:M = 4:1) and affects from 10 – 25% of the general population and up to 35% of patients with leg length discrepancies and low back pain. Additional risk factors include abnormal hip biomechanics, ipsilateral iliotibial band (ITB) pain, knee osteoarthritis, obesity and specific sporting activities (Del Buono et al, 2011, p. 2). The physical examination of a patient with GTPS characteristically reveals point tenderness in the posterolateral area of the greater trochanter typically at either the site of the gluteus medius tendon insertion or the insertion of the gluteus minimus tendon. Pain can also be reproduced through active resistance to abduction and external rotation and sometimes by internal rotation of the hip (Williams & Cohen, 2009, p. 1665). The most valuable diagnostic studies for GTPS include Computed Tomography (CT) and Magnetic Resonance Imaging (MRI) with partial thickness and complete thickness tears of the gluteus minimus or medius tendons visible on MRI. X-rays of the hip may show evidence of associated musculoskeletal conditions, calcifications and irregularities around the greater trochanter, however they generally have little diagnostic value for GTPS (Geraci et al, 2011, p. 77) Conservative treatment measures include rest, anti-inflammatory medication, ice, weight loss, stretching and strengthening exercises, physical therapy and ultrasound. These interventions aim to improve flexibility, muscle strength and joint mechanics whilst decreasing pain. When these interventions fail, bursa or lateral hip injections performed with corticosteroid and local anaesthetics are performed. For patients who fail to respond, surgical intervention is advocated with arthroscopic bursectomy and/or ITB release performed (Williams& Cohen, 2009, p. 1668). The Bowen Technique (also known as Bowtech and Bowenwork) is a dynamic system of muscle and connective tissue therapy developed by the late Tom Bowen in Geelong Australia. It is a gentle form of soft tissue therapy used in the relief of many specific injuries and other health problems, both acute and chronic. (Rentsch 2007 p. vii) The Bowen Technique addresses the body in a holistic manner. The practitioner delivers signals to the nervous system via sets of moves at specific locations (muscles, tendons, ligaments and nerves), then allows the body time to respond with subtle adjustments in tension, prior to performing the next set of moves (Bowtech, 2009). The basic Bowen “move” distorts a muscle or tendon that is not under load and then rolls over it at a precise location without sliding on the skin. As a result, the spindle cells and Golgi tendon organs down-regulate the muscle’s resting tension level via the central nervous system. The surrounding fascia becomes less solid and more fluid, allowing greater movement of blood and lymph through the tissue, and enhancing nutrition to and waste removal from the site of injury. The lack of distracting skin stimulation and the limited number of precise moves focus the nervous system’s attention on the essential points. Diploma – Specialised Bowen Therapy Michelle Mauro Page 4 of 12 Pausing at certain crucial times in a sequence of such moves allows time for the nervous system and fascia to respond and begin the healing process (Bowtech, 2009). Demographic Statistics This research project was conducted in the Redlands, a Shire of Brisbane, Queensland. The Redland City Council demographic profile, based on results obtained from the 2011 Census of population and housing, states a population of 138 670 covering a land area of 537 square kilometres (Redland City Council, 2010). The age structure shows that: 34.8% of population is ≥ 50 years of age 32% of population is 25-49 years of age 33% of population is 0-24 years of age A search of Bowen practitioners on the Bowen Association of Australia and Bowtech websites found 8 practitioners located within approximately 10 kilometres of Capalaba, a suburb within the Redland Shire, however only one of these practitioners was listed as working within the Shire. Four of the eight practitioners were located more than seven kilometres from Capalaba (Bowtech, 2009 & BAA). Lack of information, advertising and general knowledge within the community suggests little knowledge of the Bowen technique and it would appear that the lack of practitioners would make it difficult for some people to access this modality. There are however ample medical practitioners and physiotherapists within the Shire. With advice from medical practitioners, I believe that the vast majority of people would be encouraged to pursue the current medical recommendations for treatment including physiotherapy and steroid injections. Aims and Objectives of the Project The aim of this project is to: To evaluate the effectiveness of the Bowen Technique for symptom management in Greater Trochanteric Pain Syndrome (GTPS). Research Methods/Strategies Both qualitative and quantitative research methods were used in this study. Subjective assessment was employed with the client interviewed regarding symptoms and pain levels. Objective assessment was performed through active, passive and resisted movements Diploma – Specialised Bowen Therapy Michelle Mauro Page 5 of 12 followed by specialised tests. Pre and post therapy semi-structured interviews of patient, including personal perceptions of therapy were also conducted. Study Sample/Stakeholders This project focussed on the treatment of GTPS in one female client, 44 years of age. Relevant medical history includes fractured right ilium age 11. The client had experienced intermittent weakness and pain in the right hip and buttock over the previous 15 years however no therapy or investigations were conducted. Client has had three problem free, full term pregnancies. Client noticed ongoing pain in the right hip approximately 3-4 months prior to presentation for Bowen Therapy. The pain was continual and was exacerbated when running, walking up stairs and for long periods of time or lying on the affected side. The pain levels ranged from 4-9 on a pains scale of 1 to 10 and analgesics were required on a regular basis to ensure a full night’s sleep. Diagnostic x-rays showed no obvious abnormalities and physiotherapy was recommended by her general practitioner who diagnosed Greater Trochanteric Pain Syndrome. The GP also suggested corticosteroid injections into the lateral hip should the condition not respond adequately to physiotherapy. No other treatments were undertaken for the condition. The client was recommended Bowen Therapy by a relative who had experienced excellent results for a different condition. With minimal response to physical therapy, the client had no therapies for approximately two months prior to presenting for Bowen Therapy. Ethical Considerations The client was invited to participate in a research study and was given verbal information on the research project in addition to a participation information sheet and consent form for their consideration. Bowen Therapy, its history and effect on the body were discussed at length and all questions answered to the client’s satisfaction. Information relating to client confidentiality and publishing of results was also discussed. Please refer to Appendix 1 for client information sheet and consent form used. Data Collection – Results Subjective Assessment On initial presentation, right hip pain experienced was 9 on a pain scale of 1 to 10. Pain was radiating down the right lateral thigh with the feeling of weakness present in the right buttock and hip area. Client had difficulty walking up stairs, could not run or participate in vigorous exercise and could not walk for any length of time. She was unable to sleep on her right side Diploma – Specialised Bowen Therapy Michelle Mauro Page 6 of 12 and experienced interrupted sleep due to hip pain. The pain was continual throughout the day and evening and ranged from 4 to 9 on a pain scale of 1 to 10. The client initially had no knowledge of the Bowen Technique and had very limited expectations regarding its effectiveness for the treatment of her condition. She had gained minimal to no benefit from physiotherapy sessions and felt reluctant to continue with this modality due to the pain and discomfort experienced during the sessions. At the urging of a family member she attended Bowen Therapy as she was reluctant to proceed with corticosteroid injections as recommended by her general practitioner. The client experienced a full, uninterrupted night’s sleep following the first session, however, there was minimal improvement in symptoms and the second session was conducted five days later due to high levels of pain. Following the second session, the client experienced a gradual but continual decrease in pain and symptoms. By the fifth Bowen Therapy session, no pain was experienced in the objective testing; the client was experiencing uninterrupted sleep and had started walking her dog for a half an hour each day – something she had been unable to do for the previous three months. Increased right leg strength and greater range of movement in the right hip was noted at the fourth and fifth therapy sessions. Objective Assessment: On palpation, from the posterior view, the right iliac crest was noted to be approximately 1.5 – 2cm higher than the left at the first therapy session. Both crests were level at session 5. No pain was experienced with active lumbar movements. Active movements of the knee were negative for pain. Active Testing Bowen Session 1 2 3 4 5 Hip Supine Pain Right hip on abduction ROM – 20º. Pain Right hip on abduction ROM – 25º. Pain Right hip on abduction ROM – 30º. Pain Right hip on abduction ROM – 40º. Stop P1 Stop P1 Stop P1 Stop P1 No Pain all movements. Abduction ROM - 40º Stop R1 Bowen Session 1 2 3 4 5 Hip Supine No pain in all movements. Stopped at S1 No pain in all movements. Stopped at S1 No pain in all movements. Stopped at S1 No pain in all movements. Stopped at S1/R1 No pain in all movements. Stopped at S1/R1 Passive Testing Diploma – Specialised Bowen Therapy Michelle Mauro Page 7 of 12 Resisted Tests Bowen Session 1 2 3 4 5 Hip Flexion No pain. Weakness in right leg No pain. Weakness in right leg No pain. Weakness in right leg No pain. Slight weakness right leg No pain. Slight weakness right leg Hip Extension No pain. Weakness in right leg No pain. Weakness in right leg Slight discomfort. Weakness in right leg Slight discomfort. Slight weakness right leg No pain. Slight weakness right leg Hip Abduction Pain in right hip. Weak response right leg Pain in right hip. Weak response right leg Slight discomfort. Weakness in right leg Slight discomfort. Weakness in right leg No pain. Slight weakness right leg Hip Adduction Pain in right hip. Weak response right leg Pain in right hip. Weak response right leg Slight discomfort. Weakness in right leg Slight discomfort. Weakness in right leg No pain. Slight weakness right leg Special tests conducted included Ober test which showed a slight positive on the right leg and Thomas test which demonstrated a negative result. No leg length, tibial length or femur length discrepancy was noted. Procedures Used BT Session 1 2 3 4 5 Procedures Used BRM 1, 2, 3, H/S & Head BRM 1, 2, H/S, Pelvic, Knee BRM 1, 2, H/S, Coccyx, Pelvic, Knee BRM 1, 2, H/S, Coccyx Obl, Pelvic, Knee BRM 1, 2, H/S, Coccyx Obl, Pelvic, Knee, Ankle, H/T & Bun Client was given Bowen Hamstring and Pelvic exercises following week 2. The client built up to these slowly and only to her level of comfort. Data Analysis – Conclusion The initial Bowen treatment was used to relax and balance the body with subsequent sessions specifically addressing the muscles and tendons within the pelvic and hip area. It was noted that the client had an inverted coccyx and the coccyx and coccyx oblique procedures were used throughout sessions three to five. Diploma – Specialised Bowen Therapy Michelle Mauro Page 8 of 12 The client reported immediate relief and a good night’s sleep following the first session however pain levels increased approximately two to three days following this. Client interviews demonstrate a continual, gradual decrease in pain and symptoms over Bowen sessions two to five. This is in line with results of subjective and objective assessment which indicated a gradual decrease in pain, greater range of movement and increase in strength through the right buttock and leg. Following the fifth treatment session, the client experienced no symptomatic pain and was participating fully in everyday activities. This was a pleasing result for the client considering the negative impact GTPS was having on her life. The client is convinced that resolution of her symptoms is a result of the Bowen Technique as she did not change her lifestyle or receive other therapies whilst receiving Bowen Therapy. She is currently on a maintenance program and attends Bowen sessions once per month. Although this study was conducted on a single subject, the results were very positive and encourage further investigation into the use of the Bowen Technique for symptomatic relief of GTPS. There are medical practitioners and allied health professionals who are open to results obtained from case studies in therapies outside their realm of practice, however the wider healthcare community often require evidence before changes to treatment recommendations are made. To confirm and establish the Bowen Technique as an effective therapy for GTPS, further research is required in the form of feasibility studies and controlled trials to provide an evidence base for changes to current established treatments. Sharing Knowledge Many people in the wider community experience lateral hip pain diagnosed as Greater Trochanteric Pain Syndrome resulting from acute or repetitive trauma. As Bowtech practitioners, we do not diagnose, however it is valuable to have knowledge of the presenting conditions experienced by the client. In addition to causes and risk factors, this information enables us to understand the link between musculoskeletal anatomy and symptoms, allowing the formulation of a treatment plan that aims to provide the best outcome for the client. It is the intention of this research article to educate Bowtech practitioners, and subsequently their clients, on the signs, symptoms, risk factors and treatment options for GTPS and investigate and share the results obtained from the use of Bowen Therapy as a treatment option. Appendix 1 PARTICIPANT INFORMATION SHEET Diploma – Specialised Bowen Therapy Michelle Mauro Page 9 of 12 1. Invitation You are invited to take part in a research study. Please take time to read the following information carefully and to decide if you wish to take part in the study. Feel free to ask if there is anything that is not clear or if you would like more information. 2. What is the purpose of this clinical research study? The purpose of this study is to investigate whether the use of the Bowen Technique results in the relief of symptoms for Greater Trochanteric Pain syndrome (GTPS). 3. What does this study involve? Participation in Bowen Therapy treatment sessions that include answering questions regarding your: Medical history Lifestyle and physical activity & sleep patterns Pain level and the effects of GTPS on your everyday activities Understanding and perception (if any) of the Bowen Technique. These questions will take approximately 15 minutes. Your participation in this study is voluntary and you can withdraw at any time. 4. Treatment You will meet with your Bowen therapist weekly for 3 consecutive weeks. These appointments will take approximately 1 hour. The timing and number of follow-up treatments will be discussed with you and be according to response to treatment. No other therapies are to be undertaken during the Bowen course of treatment. 5. What are the Possible Benefits from participating in this study? Possible benefit of participation in this study is reduction or complete resolution of symptoms associated with GTPS. However benefit is not guaranteed. Other Bowen therapists and people with GTPS may benefit in the future from knowledge gained from this research study. 6. How will my confidentiality be protected? Any identifiable information that is collected about you in connection with this study will remain confidential and will be disclosed only with your permission, or except as required by law. 7. What will happen with the results of the study? The results of the study will be presented to Border College of Natural Therapies for review and presented to peers to share knowledge gained. 8. Further information and contact details Contact Details Michelle Mauro Bowen Therapist BAA Membership No. 9833 Phone No. 0437 735 708 Appendix 2 - Consent Form Diploma – Specialised Bowen Therapy Michelle Mauro Page 10 of 12 CONSENT FORM Participation in a Research Study The Use of the Bowen Technique for Symptom Relief in Greater Trochanteric Pain Syndrome (GTPS) By signing this consent form: 1. I confirm that I have read the Participant Information Sheet for the above study. I have had the opportunity to consider the information, ask questions and have had these answered satisfactorily. 2. I understand that my participation is voluntary and that I am free to withdraw at any time without giving any reason. I understand that relevant information of my medical history and data collected during the study may be looked at by individuals from Border College of Natural Therapies and I understand any identifying information will be kept confidential. Signature Clients Name: Signature: Date: Declaration by the Practitioner I hereby declare that I have discussed the purpose and procedures of this research study with the client. Practitioner Name: Signature: Date: Bibliography Diploma – Specialised Bowen Therapy Michelle Mauro Page 11 of 12 Bowen Association of Australia, “Find a Practitioner”, http://www.bowen.org.au/find-apractitioner/, 3/8/13. Bowtech: The Original Bowen Technique, (2009), “Bowen Practitioner Search” http://www.bowtech.com/WebsiteProj/Pages/Practitioner/Search.aspx, 3/8/13. Bowtech: The Original Bowen Technique, (2009), “How it Works”, http://www.bowtech.com/WebsiteProj/Pages/About/HowItWorks.aspx, 26/07/13. Brinks, A, Van Rijn, RM, Willemsen, SP, Bohnen, AM, Verbaar, JA, Koes, BW & BiermaZeinstra, SM (2011), “Corticosteroid Injections for Greater Trochanteric Pain Syndrome: A Randomized Controlled Trial in Primary Care”, Annals of Family Medicine, Vol. 9, No. 3, pp. 226-234. Del Buono, A, Papalia, R, Lhanduja, V, Denaro, V & Maffulli, N (2011), “Management of the greater trochanteric pain syndrome: a systematic review”, British Medical Bulletin 2011, pp. 1-17. Geraci, A, Massoccato, G, Gasparo, M (2010), “Greater Trochanteric Pain Syndrome: What is this Meaning?”, Timisoara Medical Journal, Vol. 61No. 1-2, pp. 74-79. Klauser, AS, Martinoli, C, Tagliafico, A, Bellmann-Weiler, R, Feuchtner, GM, Wick, M & Jaschke, WR (2013), “Greater Trochanteric Pain Syndrome”, Seminars in Musculoskeletal Radiology, Vol. 17, no. 1, pp. 43-47. Mechner, V (2003), “The Bowen Technique”, http://www.bowtech.com/WebsiteProj/documents/1666-MechnerMassage%20Magazine%20Article.pdf, 3/8/13. Redland City Council, (2010), “Demographic Profile”, http://www.redland.qld.gov.au/AboutRedlands/DemographicProfile/Pages/default.aspx, 3/9/13. Rentsch O & Rentsch E (2007) Bowtech Instruction Manual Modules 1 & 2, Bowtech Pty Ltd, Hamilton. Segal, NA, Felson, DT, Torner, JC, Shu, Y, Curtis, JR, Niu, J & Nevitt, MC (2007), “Greater Trochanteric Pain Syndrome: Epidemiology and Associated Factors”, Archives of Physical Medicine & Rehabilitation, Vol. 88, pp. 988-982. Williams, BS & Cohen, SP (2009), “Greater Trochanteric Pain Syndrome: A Review of Anatomy, Diagnosis and Treatment”, International Anasthesia Research Society, Vol. 108, no. 5, pp. 1662-1670. Diploma – Specialised Bowen Therapy Michelle Mauro Page 12 of 12