Clinical Endodontic Diagnosis
advertisement

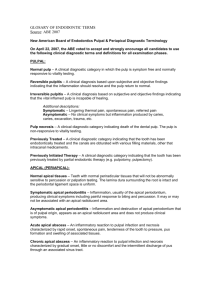
Clinical Endodontic Diagnosis Robert S. Roda DDS MS Basic Principles of Endodontics •Clean, shape and obturate the root canal systems •Restore the tooth and re-establish the occlusion How to Achieve Endodontic Success •Accurate diagnosis •Good access •Thorough cleaning and shaping •Effective obturation •Quality restoration Clinical Endodontic Diagnosis “There may be different ways of treating a disease, however there can be but one correct diagnosis” Morton Amsterdam 1974 Diagnostic Objectives •Reproduce the Chief Complaint •Determine the Cause •Eliminate the Cause Case #1 •The Patient –28 y.o. female –Caucasian –Office worker –She is obviously in pain –She is holding a cup of ice water –She doesn’t look as if she’s slept well. –What’s going on with this patient? •Subjective Information •Objective Findings •Assessment •Plan of Treatment History •Chief Complaint –“What problem can I help you with, today?” (Write the response in the chart under chief complaint) –“I have a toothache.” History Medical History Form •Completed by patient •Signed and dated •Reviewed completely •Follow-up questions •Highlight significant conditions Case #1 - History •Medical History –Generally good health –Had rheumatic fever as a child –Allergic to pennicillin S.O.A.P. •Subjective Information –History of Pain –Stimulus of Pain –Severity of Pain –Frequency of Pain –Duration of Pain –Location of Pain –Spontaneity of Pain Subjective Information •History of the pain –When did it start? –Was the pain related to a specific experience? •Recent dental treatment •Trauma •No specific incident •Stimulus of the pain –Cold / Heat –Biting / Chewing / Touching / Pressure –Pushing on the gums –No stimulus •Severity of the pain –Scale of 1 to 10 –1 = no pain –10 = worst pain imaginable –Subjective patient judgment •Frequency of the pain –Intermittent or continuous? –How often do episodes occur? –Related to some stimulus? Duration of the pain –How long does it persist after removing the stimulus? •0 – 30 seconds •> 30 seconds –Never stops •Location of the pain –Localized to one tooth –Poorly localized to one quadrant –Poorly localized to one side of the face –Poorly localized to both sides of the midline •Spontaneity of the pain –Spontaneous •No stimulus related to it •Wakes patient up at night –Non-spontaneous •Always needs a stimulus •Does the stimulus always cause the pain? •Nature of the pain –Throbbing, burning, shooting, dull, sharp –Very subjective descriptors Case #1 •Subjective Information –Pain started on it’s own three days ago - worsening –Pain is a spontaneous, constant throbbing –Pain worsens when ingesting hot substances, lingers –Pain is relieved by cold –Pain is slightly worsened by biting –Pain feels like 9 out of 10 - wakes patient up at night •Document Everything! S.O.A.P. •Objective Findings –Clinical Examination •Extraoral •Intraoral –Radiographic Assessment –Comparative Testing –Document Everything! •Objective Findings –Clinical Examination –Radiographic Assessment –Comparative Testing •Clinical Examination •Visual Exam / OCS Palpation • Percussion • Presence of a Sinus Tract / Swelling • Caries • Tooth Fractures • Fractured or Extensive Restorations • Periodontal Disease / Probing / Mobility • Exposed Dentin • Wear Facets S.O.A.P. •Radiographic Assessment •Buccal Object Rule • Case #1 •Radiographic Assessment Clinical Tips •Images –Must be current –Must be complete •Palpation –Get patient accustomed to “normal” –Work towards suspect tooth •Percussion –Start with uninvolved teeth •Perio probe – What is WNL? •Mobility –Slight - Moderate – Extensive –Grade I, II, III (vertical) •Objective Findings –Comparative Testing •Thermal Tests –Cold (H2O, CO2, Endo Ice) –Heat (Warm Gutta Percha) •Bite Test •Electric Pulp Test •Transillumination •Anesthetic Test –Injection –Topical •Test Cavity Clinical Tips •Cold –Blowing air is inaccurate –Use Endo Ice, ice stick, or CO2 snow •Heat –Use dab of petroleum jelly to keep gutta percha from sticking to tooth •Anesthetic Test – may anesthetize adjacent teeth •Cavity Test – patient reluctance S.O.A.P. •Assessment –Pulpal Diagnosis –Periradicular Diagnosis –Non-Endodontic Pathology •Pulpal Diagnosis Reversible Pulpitis - Non-lingering (Thermal tests) Not spontaneous. Usually does not require RCT Irreversible Pulpitis (symptomatic) – Spontaneous pain. Lingers (after stimulus or thermal tests). Usually severe pain Usually requires RCT Irreversible Pulpitis (asymptomatic) – no clinical symptoms but irreversible pulpal inflammation is produced by caries, caries excavation, trauma, etc. Usually requires RCT Pulp Necrosis - No Response to thermal or electrical stimuli Usually requires RCT Previous Root Canal Therapy –previously completed root canal (canals are obturated) Usually requires RCT if disease is present or likely to develop Previously Initiated Therapy - previous pulpotomy/pulpectomy where treatment is not complete, but the canal may contain intracanal medicaments •Periradicular Diagnosis Normal Apical Tissues Symptomatic Apical Periodontitis - pain to biting and percussion (sometimes severe). May or may not have an apical radiolucency Asymptomatic Apical Periodontitis - Cannot elicit pain or altered sensation, apical radiolucency present Acute Apical Abscess - Localized Swelling, pain and pus formation associated with a necrotic and infected pulp. Fever, lymphadenopathy, and periapical radiolucency may or may not be present Chronic Apical Abscess - Inflammatory reaction to pulpal necrosis and inflammation characterized by mild or no symptoms and pus draining from a sinus tract. Cellulitis - Extraoral spread of infection. Dangerous – treat aggressively •Non-Endodontic Pathology –Acute Periodontal Abcess –Vertical Root Fracture –Acute / Chronic Sinusitis –TMD / MPD (incl. Occlusal Trauma) –Neuropathic Pain –Vascular Pain –Atypical Facial Pain