ONLINE APPENDIX: IV. Residual Perthes deformity with acetabular
advertisement

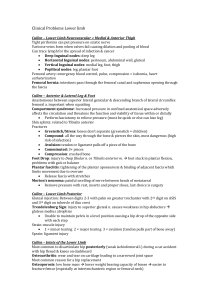
ONLINE APPENDIX: IV. Residual Perthes deformity with acetabular dysplasia A 16-year-old female, highly competitive soccer player, with a history of Perthes disease treated with PFO eight years prior, presented to our clinic with right hip pain. Physical examination revealed a positive Trendelenberg sign and a limb length discrepancy of 1 cm with the right being short. Her right hip range of motion was 0 to 95, with an IRF of 0, ERF of 5, and abduction of 15 degrees. Anterior impingement testing was also positive. Radiographs demonstrated coxa magna, coxa breva, coxa vara, and a prominent greater trochanter, in addition to acetabular dysplasia and retroversion (Figure 7). Surgical hip dislocation revealed an aspherical femoral head with an anterior and anterolateral prominence, an area of labral degenerative tear, and diffuse chondromalacia of the femoral head. A femoral head/neck junction osteochondroplasty was performed, followed by a relative femoral neck lengthening and trochanteric advancement of 1 cm. The degenerative labral tear was treated with debridement. The hip had dramatic improvement in motion, however in flexion and adduction was unstable. A PAO was therefore performed (Figure 8A). The patient had her trochanteric screws removed at approximately 1-year from the surgical dislocation, and is pain free and has returned to full activity (Figure 8B). She has improvement of range of motion from 0 to 95, IRF to 10, ERF to 10, and abduction to 20, degrees. V. Posttraumatic A 12-year-old male previously sustained a displaced femoral neck fracture that was treated with open reduction and internal fixation with three 6.5 mm cannulated screws. He subsequently developed avascular necrosis with femoral head collapse and extrusion. Hardware removal was then performed. He presented one year after his injury with worsening pain, stiffness, and limited function. Hip flexion was from 0 to 80 degrees, with an IRF of 10, and ERF of 10, and abduction of 10 degrees. Radiographs demonstrated osteonecrosis with central femoral head collapse and extrusion of a lateral femoral head fragment (Figure 9). Fluoroscopic examination under anesthesia revealed that the posteromedial femoral head was the most congruent with the acetabulum, and a valgus and flexion femoral osteotomy was therefore recommended. Surgical dislocation was performed revealing a severely malformed femoral head with extrusion of the anterolateral head/neck junction. There was diffuse chondromalacia of the femoral head and acetabulum. Recontouring of the head/neck junction was performed to relieve impingement anteriorly and anterolaterally, which was severe especially in abduction as well as flexion and internal rotation. There were areas of sclerosis, but in general the femoral head displayed good blood supply with bleeding via the cut surfaces. The osteochondroplasty resulted in marked improvement in the range of motion and relief of the intra-articular impingement. A proximal femoral osteotomy was then performed with blade plate fixation, with approximately 10 degrees of valgus and 25 degrees of flexion correction, resulting in additional improvement of hip flexion, abduction, and internal rotation in flexion. The patient elected to have the blade plate removed and at 1½ years from the surgical dislocation and has major improvement in symptoms, activity, with return to basketball (Figure 10). He has improvement in range of motion from 0 to 90, IRF to 10, ERF to 20, and abduction to 40 degrees. VI. Residual deformity after SCFE treated with SD and PFO A 12-year-old female with a history of bilateral SCFE’s treated with in-situ pinning 2 years prior, presented with left hip pain. She subsequently had her hardware removed, but continued to complain of left hip pain, with mechanical symptoms, and restricted motion. Her left hip range of motion was 0 to 55 degrees with obligate external rotation, with an IRF of -10, and ERF of 75 degrees. Anterior and lateral impingement testing and Patrick’s FABERs was also positive. Radiographs revealed a posteriorly displaced femoral head with a prominent anterolateral head/neck junction, which showed a clear impingement trough, in addition to a high greater trochanter in relation to the center of the femoral head (Figure 11). Surgical dislocation of the hip revealed major impingement of the femoral headneck junction in flexion and internal rotation. There was diffuse femoral head chondromalacia and focal superolateral acetabular chondromalacia with a partialthickness cartilage flap, in addition to an anterior and superolateral labral tear measuring approximately 25-mm. Recontouring of the femoral head-neck junction was performed followed by a relative femoral neck lengthening, greater trochanteric advancement, and resection of the superior greater trochanter to treat the extra-articular impingement. A minor acetabular rim trimming was performed followed by repair of the acetabular labral tear and debridement of the acetabular chondral flaps. A proximal femoral osteotomy was then performed with approximately 30 degrees of flexion and 20 degrees of internal rotation correction, which was fixed with a blade plate (Figure 12) The patient is approximately 1-year from the surgical dislocation with improvement in symptoms and activity. She had improvement of range of motion from 0 to 90 degrees, IRF to 5, and ERF to 45 degrees. Her modified Harris hip score improved from 85 to 100. Figure 7. Perthes disease with acetabular dysplasia. A. AP pelvic radiograph demonstrated a Perthes type hip with coxa magna, coxa breva, coxa vara, and a prominent greater trochanter. This also decomstrates acetabular retroversion (cross-over sign) and dysplasia with a diminished lateral center edge angle and elevated acetabular index. B. False profile radiograph also demonstrated diminished anterior center edge angle. C, D. Dunn view and frog-leg lateral also reveals the aspherical deformity present. Axial (E) and sagittal (F, G) T2 MR arthrogram images demonstrate an anterior and superolateral degenerative labral tear (arrowhead). Figure 8. A. AP radiograph demonstrating correction of the femoral head/neck offset, trochanteric height, and acetabular dysplasia. B. After removal of hardware demonstrating full osseous union of the trochanteric and pelvic osteotomies. Figure 9: Post-traumatic avascular necrosis. A, B. AP pelvis and false profile radiographs revealed central femoral head collapse and extrusion of an anterolateral femoral head fragment. C, D. Frog-leg lateral and Dunn views demonstrate diminished head/neck offset and impingement. 3-dimenstional (E) and an axial slice (F) CT scan again demonstrated the central femoral head impaction (*) and lateral extrusion with a preserved posteromedial femoral head (arrowhead) Figure 10: A,B,C. Post-operative radiographs demonstrating improvement of the femoral head sphericity, and increased femoral head/neck offset. D. AP radiograph after removal of prominent hardware demonstrating preservation of the hip joint, two years after the reconstruction. Figure 11. Residual SCFE. Radiographs demonstrate a posteriorly displaced femoral head with a prominent anterolateral head/neck junction, with an impingement trough (arrow), in addition to a high greater trochanter in relation to the center of the femoral head. Figure 12. A, B. Restoration of the femoral head/neck offset in addition to the trochanteric height. C. Removal of the prominence from the head/neck junction. D. Relative femoral neck lengthening. E. Labral repair.