Fitzakerely_-_Motor_Control
advertisement

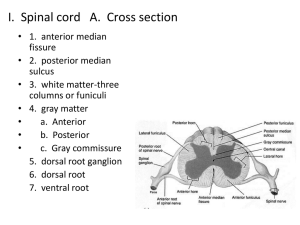
Fitzakerely – Motor Control – NS Exam 2 1. List the general categories of movements, and be able to rank them with respect to the degree of supraspinal control. Be able to give an example of each type of movement. 1. Reflex: fixed, automatic response (triggered by very specific stimulus) very rapid event (very few synapses) like 10 (v. 1000s) little voluntary control, but you can modulate them Ex: patellar tendon reflex, stretch reflex 2. Postural: upright (wrt gravity) Combination of reflexes + volition (decision making) Ex: vestibulospinal reflexes (Inner ear Spinal Cord) 3. Rythmic: Also combo of reflexes + volition o Initiation is voluntary but mvmt itself is sterotyped Ex: walking, running, chewing 4. Voluntary: purposeful, goal directed Initiated by CNS Improve with practice Most movements involve GROUPS of muscles (agonists & antagonists) All systems ultimately synapse on α motoneuron But really…that path isn’t ‘final’ o there is constant feedback from sensory receptors that monitor how process is going so that CNS can adapt to changing force needs 2. Outline the structures involved in the planning, initiation and execution of voluntary movements. Understand how these structures are interrelated. 3. List the components of a reflex arc. Identify ways that a reflex can be modulated, and understand (in general terms) how adding or removing descending inputs can change reflex functions (particularly the stretch reflex). Relex arc – basic unit of integrated reflex activity: o sensory receptor o afferent neuron o one or more synapses in CNS o efferent neuron o effector 4. Understand the physiology of: flexor withdrawal and crossed extension reflexes, recurrent and reciprocal inhibition, clonus, magnet reaction, mass reflex, Babinski sign. MONOSYNAPTIC REFLEXES: afferent neuron synapses directly on the efferent neuron POLYSYNAPTIC REFLEXES: paths branch in a complex way o synaptic delays mean that activity in the branches with fewer synapses reaches the motor neurons first, followed by activity in the longer pathways o a single stimulus can cause prolonged "waves" of response o some branches can turn back on themselves, allowing activity to be terminated through the process of RECURRENT INHIBITION a well-known example is that of Renshaw cells, inhibitory interneurons that are activated by axon collaterals of motor neurons - once activated, a Renshaw cell inhibits the motor neuron that stimulated it, as well as other neighboring motorneurons that innervate agonist muscles Withdrawal reflex: polysynaptic reflex occurs in response to noxious (usually painful) stimulation o response is contraction of flexor muscles and o inhibition of extensor muscles, so that stimulated part is withdrawn from the stimulus o this occurs through the process of RECIPROCAL INHIBITION: collateral branches of the Ia afferent fibres synapse on inhibitory interneurons that suppress the activity of alpha motor neurons that innervate antagonist muscles if the part is a limb, the response includes extension of the opposite limb (the crossed extensor response) o the spread of excitatory impusles up and down the spinal cord to activate more motor neurons is called irradiation of the stimulus, and this process results in recruitment (it results in an increase in the number of active motor units) stronger stimuli produce greater flexion and shorter reaction times, sometimes producing a series of movements due to prolonged, repeated firing of the motor neurons (after-discharge) Spinal shock: spinal cord transaction results in paraplegia, and loss of sensation in body parts innervated by spinal segments below the lesion duration of spinal shock is proportionate to the degree of cortical control of motor control systems o in frogs/rats, it lasts minutes; dogs/cats 1-2 hours; monkeys days; humans, at least 2 weeks, sometimes weeks or years causes of spinal shock are unknown, but it may involve loss of descending synaptic facilitation o can prove that it is loss of descending control, by performing (in animals) a 2nd transection below the original lesion; there is no spinal shock in response to the 2nd transection reflex responses eventually return, and become hyperactive; the following signs appear in order: 1. noxious stimulus of the sole of the foot produces movement of the toes, resulting eventually in a Babinski sign (Normal is plantarflexion) 2. noxious plantar stimulation or tactile stimulation of the perianal skin contraction of the spincter ani 3. genital reflexes (erection and ejaculation) 4. flexor withdrawal activity in the foot and ankle, eventually resulting in a mass reflex (a minor stimulus causes bladder and bowel evacuation, sweating, pallor & changes in BP) 5. flexor withdrawal activity from larger areas of the limb at lower threshold, that can result in spasms (painful) 6. reflex activity involving extensor muscles extensor spasms clonus: regular rhythmic contractions of muscle when stimulated clasp knife reflex & crossed extension reflex hyperactive stretch reflexes, including the magnet reaction (occurs in babies b/c descending circuitry doesn’t come down to suppress) the flexor spasms can be associated with bursts of pain o treatment with BACLOFEN, a GABAB receptor agonist, inhibition and reduces the spasms 5. Distinguish between alpha and gamma rigidity, and between decorticate and decerebrate rigidity. Understand the effects on alpha and gamma motorneurons in each case decerebration reveals the tonic, static postural reflex mechanisms maintained by the: o brain stem reticular formation facilitates gamma motor neuron activity o vestibulospinal system facilitates alpha motor neuron activity (not abolished by deafferentation) the pattern in true decerebrate rigidity is extension in all four limbs o similar to what is seen in 4-legged animals (we are not far enough removed from our quadruped ancestors to have changed the pattern of brain stem activation of our upper extremeties, even though the main antigravity muscles in the arms are flexors) no phenomena akin to spinal shock, as rigidity occurs as soon as the brain stem is transected spasticity is due to diffuse facilitation of stretch reflexes due to: o increased excitability of the motor neuron pool (alpha rigidity) independent of stretch reflex pathways o increase in the discharge rate of gamma efferent neurons (gamma rigidity) dependent on stretch reflex pathways progression from decorticate to decerebrate rigidity is an ominous sign, as it indicates that the lesion is progressing from the cortex to the brainstem, and decerebration is usually fatal; elimination of the brainstem and vestibulospinal inputs causes the muscles to become flaccid (as the patient dies) o true decerebration is rare in humans removal of the cerebral cortex causes a severe motor deficit, although movement is still possible moderate rigidity is present due to loss of inhibition of gamma motor neurons only seen at rest, due to the presence of postural reflexes patients present with flexion of the upper extremities at the elbow, and extension of the lower extremities