Downloadable Patient History Form
advertisement

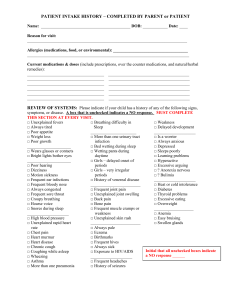
Allergy and Weight Loss Center (Concord Weight Loss Clinic) Weight and Nutrition History Name: ___________________________ Date of birth: ______________ Today’s Date: _________ Primary Physician: __________________ How did you hear about our program? _________________ Maximum lifetime weight:_____________ Desired weight:_____________ Please circle all that apply: How long you have been overweight? Since childhood > 5 years < one year What situation led to your weight gain? Stress, college, divorce, career change, pregnancy, menopause, medications, other________________ What weight loss methods have you tried before? Diet pills, Weight watchers, Surgery, Other________ Dietary history: (please list typical meals) Breakfast: _____________________________________________________ Lunch:________________________________________________________ Dinner:________________________________________________________ Snacks:________________________________________________________ Night eater?____________________________________________________ When is the hungriest time of your day? Morning Afternoon Evening How many times a week do you eat out? _______________ What type of food? Chinese, Fast foods, Indian, Italian, Mexican, other______________ How many sodas, diet sodas per day? ____________ Exercise and activity: Inactive (sedentary)_____ Light activity_____ Moderate activity_____ What type of activity do you do now? _________________________________________ Sleep: Do you suffer from sleep disturbance? Explain____________________________ Current Medications and Dosages: Allergies to medications: ___________________________ Indicate if you or your family has a history of the following conditions: You Family Member You Diabetes Sleep Apnea High blood pressure Asthma/COPD High cholesterol Heartburn Stroke Eating disorder Heart Disease Arthritis Thyroid disease Other Cancer Other Family Member Personal History: Who lives at home besides you?_________________________________ Highest degree of education_____________________ What is your occupation?_________________ Are you: Single____ Married____ Domestic partnership____ Divorced____ Widowed____ Smoking: Currently smoking____ Amount?____ Never smoked____ Quit smoking ____ When?____ Alcohol: Yes /No How many drinks per week? ______ Are you sexually active: Yes/No Use birth control? Yes/No Are you trying to conceive? Yes/No Review of systems: (circle all that apply) Constitutional Fever Chills Weight loss Skin Itch Eyes: Vision change Pain Swelling Redness Discharge Light sensitivity Contact lens Ears: Itch Pain Nose/Throat/Neck: Itch Congestion Heart Chest pain Lungs: Cough GI: Heartburn GU: Difficulty/pain on urination Musculoskeletal: Pain Endocrine: Heat/cold intolerance Hair loss Unusual thirst Skin pigment change Sweating CNS: Seizure Dizziness Weakness Loss of balance Sleep problems Headaches Memory loss Men: Erectile dysfunction Women: Hot flashes Skin infection Weight gain Nail infection Dry Discharge Drainage Palpitations Wheezing Stretch marks Hearing loss Fatigue Acne Night sweats Rash Chronic infections Difficulty/painful swallowing Voice change Pain Swelling in feet Shortness of breath Nausea/vomiting Diarrhea Stiffness Appetite change Coughing up blood Constipation Blood in urine Numbness/tingling Snoring Abdominal pain Blood in stool Excessive urination Leaking urine Swelling Loss of sex drive Breast enlargement Testicular pain/swelling Vaginal dryness Irregular periods Dark hair growth on face/chest/abdomen Weight Loss Resistance Questionnaire Do you… Yes No Metabolic switch/Insulin Resistance/Carb Sensitivity… Frequently crave sugar? Have mood swings or energy fluctuations that influence your eating? Gain weight in your upper body/mid-section? Stress Eating… Have stress-induced cravings for salt, sugar, or fatty foods? Eat carbs after a stressful day? Food allergies… Have leaky gut syndrome? Have a history of frequent colic, ear infections, food allergies? Suffer from nasal congestion, sinusitis, asthma, hives, or eczema? Have irritable or irregular bowels? Have muscle aches, joint pains, chronic headaches? Night eating syndrome… Have sleep problems (trouble falling or staying asleep, fragmented sleep) Have daytime drowsiness? Snore? Take sleeping pills? Skip breakfast? Eat most of your calories after 5pm? Wake up to eat at night? Detoxification problems… Have fibromyalgia or chronic fatigue syndrome? Take NSAIDs (Motrin, Advil, Ibuprofen), Anti-depressants, steroids (prednisone), beta-blockers (Atenolol, Metoprolol), Psychiatric medications? For women only… Experience craving and weight gain with PMS? Have weight gain associated with menopause? ------------------------------------------------------------------------------------------------------------------------------FOR OFFICE USE ONLY: Heart Lungs Mallampati Other