Confidential - Middlebrook Family Physicians
advertisement

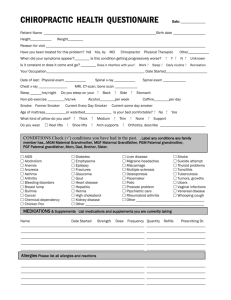
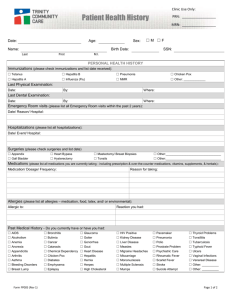
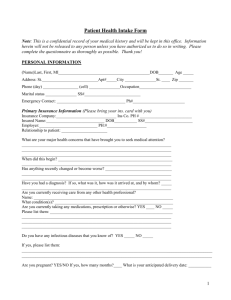
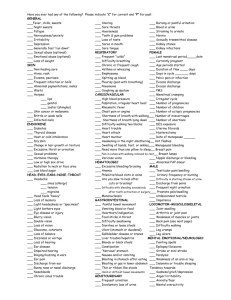
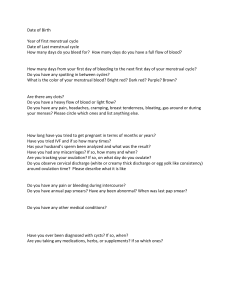
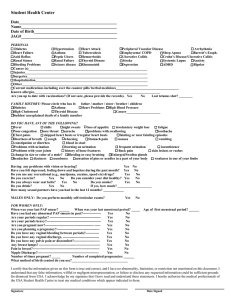
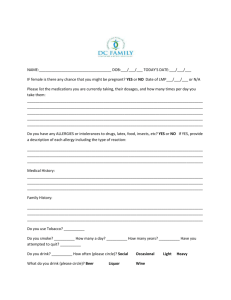
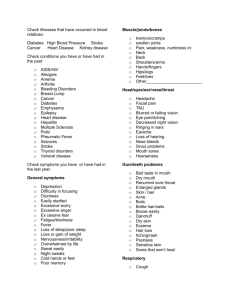
Patient Name: ______________________________________ Today’s Date: _________ Age: _______ Birth date:___________ Date of last physical examination ________ what is your reason for visit? ______________________________________ Symptoms: Check symptoms you are currently concerned with: o o o o o o o o o o o o o o o o o o GENERAL o Chills o Depression o Dizziness o Fainting o Fever o Forgetfulness o Headache o Loss of sleep o Loss of weight o Nervousness o Sweats o Muscle/Joint/Bone: o weakness/numbness in: o Arms o Back o Feet o Hands o Hips o Legs o Neck o Shoulders o Genito-Urinary o Blood in urine o Frequent urination o Lack of bladder control o Painful urination o Gastrointestinal o Appetite poor o Bowel changes o Constipation o Diarrhea o Excessive thirst o Hemorrhoids o Indigestion o Nausea o Rectal bleeding o Stomach pain o Vomiting Vomiting blood Cardiovascular Chest pain High blood pressure Irregular heart beat Rapid heart beat Swelling of ankles Varicose veins Eye, ear, nose, throat Bleeding gums Blurred vision Difficulty swallowing Double vision Ear discharge Hay fever Hoarseness Loss of hearing Nosebleeds o o o o o o o o o o o o o o o o o Persistent cough Ringing in ears Sinus problems Visions - Flashes Skin Bruise easily Hives Itching Changes in moles Sore that won’t heal MEN ONLY Breast lump Erection difficulties Lump in testicles Penis discharge Sore on penis Other WOMEN ONLY Bleeding between periods Breast lump Extreme menstrual pain Hot flashes Nipple discharge Painful intercourse Vaginal discharge Other o o o o o o o o o Last menstrual period: ___/____/________ Last Pap Smear: ___/___/____ Have you had a mammogram? Y / N Are you pregnant? Y / N Number of children: ___ List medications you are currently taking: _________________________________________________________________________________________________ Pharmacy Name: ___________________________Phone: __________________ Allergies: _______________________________________________________ Family History: Check if your blood relatives had any of the following: Disease Relationship to you Arthritis, Gout ________________ Asthma, Hay Fever ________________ Cancer and type ________________ Tuberculosis ________________ Disease Relationship to you Chemical dependency _________________ Death before age 60 _________________ Diabetes _________________ Other _________________ Hospitalizations and pregnancies: Year Hospital Reason and Outcome _______ ____________________ __________________________________________ _______ ____________________ __________________________________________ _______ ____________________ __________________________________________ _______ ____________________ __________________________________________ Year ______ ______ ______ ______ Disease Heart disease, Strokes High Blood Pressure Kidney Disease Relationship to you ________________ ________________ ________________ Hospital Reason and Outcome ___________________ ______________________________________________ ___________________ ______________________________________________ ___________________ ______________________________________________ ___________________ ______________________________________________ Health Habits: Check which you use & how much Alcohol: _______ Caffeine: _______ Tobacco: _______ Street Drugs: ________Other: _________ Occupation: ________________________________________ Check if your work exposes you to: Stress:________ Heavy Lifting: ________ Hazardous Substances: __________ Other: _____________ To the best of my knowledge, the above information is complete and correct. I understand that it is my responsibility to inform my doctor if I, or my minor child, ever have a change in health. __________________________________________________________ Signature of Patient Parent, Guardian or Personal Representative __________________________________________________________ Please print name of Patient, Parent, Guardian or Personal Representative __________________________________________________________ Reviewed By __________________________ Date __________________________ Date ___________________________ Date