stuttering updated
advertisement

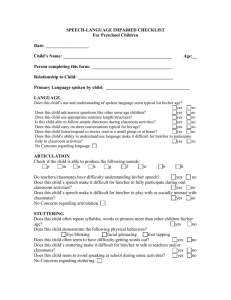
Reilly and Kefalianos September 2013 Stuttering, or stammering, is a speech disorder characterised by interruptions to speech such as hesitating, repeating sounds and words, or prolonging sounds. Around one per cent of people in all cultures stutter. In early childhood stuttering is common: 11% of children stutter at some point. Stuttering can be mild, moderate or severe, and can vary within the same individual across speaking situations and from one day to the next, particularly with children. Stuttering is graded by its degree of severity. Most researchers and clinicians rate stuttering on a 10-point severity scale. A score of 1 represents no stuttering, a score of 2 represents extremely mild stuttering and a score of 10 represents extremely severe stuttering. Stuttering can also be measured using percentage syllables stuttered whereby a speech pathologist counts all the stuttered and stutter free syllable a child says. Stuttering behaviours Stuttering behaviours vary widely between individuals, and commonly include: Hesitations, as if the next word is ‘stuck’; Repeating sounds, syllables or words such as ‘I-I-I think’ or ‘where-where-where is it?’and Prolonging sounds, such as ‘mmmm-mummy’. Origins of stuttering The cause is unknown, but researchers suspect there is a faulty connection in the area of the brain responsible for speech production. The fact that stuttering tends to run in families indicates that genetics is involved somehow in the condition. Studies of stuttering in twins have also found that both twins are more likely to stutter if they are identical rather than fraternal. Recent research found that stuttering children were not more shy or withdrawn than their non-stuttering peers. That is, personality differences did not play a role in the onset of stuttering. Reilly and Kefalianos September 2013 It was once assumed that parents played a role in the onset of a child’s stuttering. When children start to talk, they naturally hesitate and stumble over words. It was proposed that over-anxious parents believed this natural hesitation was stuttering, and pressured their child to talk properly, which caused the child to start ‘real’ stuttering. However, there is no evidence to indicate that anything parents do, or don’t do, causes the onset of stuttering. Development of stuttering Stuttering typically begins in children aged two to four years. Stuttering may develop gradually or suddenly. Stuttering can be highly variable in some children and stable in others. Impact of stuttering Older children and adults who stutter often fail to achieve their educational or career potential and may experience significant anxiety in social situations. Children who stutter report being teased by their peers. Preschool children who stutter seems to do well compared to their peers, having better receptive and expressive language skills and non-verbal cognitive performance. Preschool children who stutter were not more shy or withdrawn and did not show any evidence of social emotional and behavioural problems. Natural recovery Many children are reported to recover from stuttering or to ‘grow out of it’ without any intervention. Reports suggest this may be as high as 80%. Recovery is said to occur in the majority of children in the first 12 months after onset. However a recent study reported that just 6% of preschool children recovered during the first year after onset. Because so few children recovered the study was unable to identify factors that might predict which children might recover. An ongoing Reilly and Kefalianos September 2013 challenge for researchers is to identify factors that might separate those children who recover naturally from those who will persist and require treatment. Seek professional help Treatment is not necessary for many children close to stuttering onset. We continue to recommend a watch and wait approach. Parents should however consult a speech pathologist if they are concerned about their child’s stuttering. A speech pathologist will determine whether treatment should commence immediately or whether it is better to monitor the stuttering for a while to see if natural recovery occurs. Reports that a child is becoming unwilling to communicate or frustrated with their speech or where there are high levels of parental concern, are good reasons to instigate a referral and to commence treatment. For other children it may be appropriate to monitor the child's stuttering for a period after onset. When stuttering persists it is important to commence and to do so prior to the child starting primary school. Clinical trials have demonstrated that stuttering becomes less tractable throughout the school years. Treatment for children The best evidence (from clinical trials) for treating children who stutter is the Lidcombe Program of Early Stuttering Intervention. This is a behaviour modification treatment. Parents are trained in the Lidcombe technique. http://pediatrics.aappublications.org/content/early/2013/08/20/peds.20 12-3067.abstract?sid=69fb8a5d-b81e-474f-b9d0-08decc31d189