Emergency Contact / Health Form
advertisement

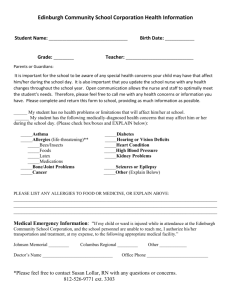
*TWO-SIDED* RETURN BY August 1, 2012 PLEASE COMPLETE ONE PER STUDENT STUDENT’S LAST NAME STUDENT’S FIRST NAME 2012-2013 Emergency and Medical Information Part A: Medical Procedures Whenever possible and prudent, the school will first notify the parent(s) and/or guardian(s) if a student has a medical emergency. Otherwise, the school will dial 911 for an emergency medical team to transport the student to a local hospital. The school will make every effort to contact the parents or guardians and give them specific information. Parents or guardians are responsible for immediately updating the Achieve website with all contact information changes, as well as updating the school’s main office of any medical conditions affecting the child. Parents or guardians are responsible for all medical and other costs affiliated with obtaining medical assistance for their child. https://cook.achieve-technology.us/login.aspx I hereby certify that I have read this document and I understand its content. Further, I assert that the health information provided to The Catherine Cook School is current and accurate. I will allow authorization to share any health information deeded necessary with applicable persons directly involved. Parent/Guardian Signature Parent/Guardian Signature Print Parent/Guardian Name Print Parent/Guardian Name Date Date Part B: Emergency Contacts If unable to reach parents/guardians, please list 3 people who you would like the school to contact in case of an emergency. Name Phone 1. 2. 3. 2012-2013 Emergency and Medical Form Alternative Phone Relationship Out of State? □ yes □ no □ yes □ no □ yes □ no Part C: Medical Information Medical Coverage Company Name Policy ID# Subscriber Name Group Physician Dentist Physician’s Phone Dentist’s Phone Medical Conditions/Medications Please complete your child’s medical health history for which school personnel need to be aware. Please list all medications (prescription and non-prescription) administered at home, if any. In addition please note any medications to which your child is known to be allergic. Finally, please list any medications to be taken at school for which a Medication Authorization Form is one file. This information allows the school to provide critical information to emergency medical technicians and care givers. Health History - Please comment on all that apply. Allergies: Hearing Impairment: High Blood Pressure: Asthma: Indigestion: ADD or ADHD: Lactose Intolerant: Chronic Illness: Learning Disability: Dietary Restrictions: Mononucleosis in past 12 Months: Emotional/Behavioral Disorder/Anxiety: Nightmares: Epilepsy/Convulsions/Seizures: Sinus Problems: Exercise-Induced Dizziness/Chest Pain: Skin Sensitivities: Diabetes: Vegetarian: Fainting/Dizziness: Visual Impairment: Additional Comments/Other: Frequent Headaches: Head/Neck/Back Injuries: Heart Disease/Defect: Prescription medications taken at home for treatment: Medication 1. 2. 3. Dose Time