Consent to Periodontal Surgical P
advertisement

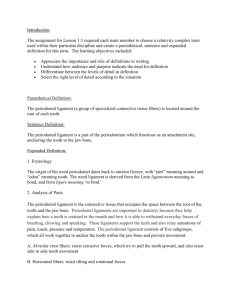
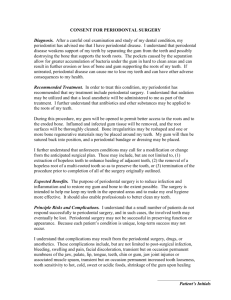
CONSENT TO PERIODONTAL SURGICAL PROCEDURES I_________________________________________, hereby authorize Norman Fine, DMD and whomever he designates as his assistant(s), to perform the following surgical treatments indicated below. _____ 1. Gingival flap surgery - open flap curettage _____ 2. Regenerative surgery - bone grafts and/or guided tissue regeneration _____ 3. Tissue repositioning - Osseous or Crown Lengthening _____ 4. Mucogingival surgery - gingival graft surgery _____ 5. Ridge Augmentation - hard tissue _____ 6. Extraction(s) _____________________________________________ 7. Other I understand that I have a form of periodontal disease/tooth loss that has caused damage to the soft tissue and/or bone around my teeth or is otherwise endangering the health of my oral tissues. This disease, if left untreated, is generally non-reversible and may be progressive, leading to further damage and possible loss of my teeth. Periodontal disease is usually controllable, but rarely curable, even with the most effective treatment. It has been explained to me that long term success of treatment requires my cooperation and performance of effective plaque control (home care) on a daily basis. It may also require periodic periodontal maintenance visits (up to several times per year) at a dental office after the proposed surgical treatment is performed. This is because most periodontal disease is chronic in nature requiring continuing treatment and monitoring to keep it under control. I further understand that if no treatment is rendered, my present periodontal condition may probably worsen in time and may result in premature tooth loss. I have been informed that other possible alternative methods of treatment include: root planing followed by periodic maintenance therapy alone, or extractions. Although significant complications from periodontal surgery are rare, they can occur. The most common complications arc as follows: Post-surgical discomfort, bleeding, swelling, tooth sensitivity, gum recession (shrinkage), increased tooth looseness, food impaction between teeth after eating, exposure of crown margins, infection, temporary or permanent nerve damage resulting in loss of sensation to lips and/or tongue, and/or tooth loss. I also understand that a variety of surgical procedures are used to treat periodontal disease/tooth loss. While these surgical procedures are generally successful, I understand that no guarantee, warranty, or assurance has been given to me that the proposed treatment will be curative and/or successful to my complete satisfaction. A risk of failure, relapse, or worsening of my present condition may result despite the treatment. 1 authorize photos or other images to be used for the advancement of dentistry and reimbursement purposes. My identity will not be revealed without my permission. I CERTIFY THAT I HAVE FULLY READ AND UNDERSTAND THE ABOVE CONSENT TO THE SURGICAL TREATMENT. I UNDERSTAND THE EXPLANANTIONS REFERRED TO, AND HAVE HAD ANY AND ALL QUESTIONS ANSWERED TO MY SATISFACTION. ALL BLANKS HAVE BEEN FILLED IN OR STRUCK BEFORE I SIGNED. DATE:_______________ PATIENT'S SIGNATURE: DATE:_______________ WITNESS" SIGNATURE: DATE: DOCTOR'S SIGNATURE: