HFD-medical-history-form - Holland Family Dentistry
advertisement

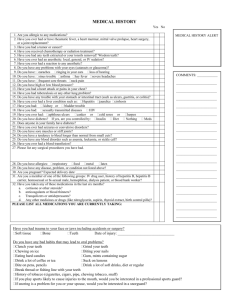
Holland family Dentistry MEDICAL HISTORY QUESTIONNAIRE Name Date of Birth Allergic to: Local Anesthetic . . . . . . . . . . . . . . Antibiotics. . . . . . . . . . . . . . . . . . . Latex. . . . . . . . . . . . . . . . . . . . . . . Other. . . . . . . . . . . . . . . . . . . . . . . Age Occupation Answer Yes or No (check appropriate box) Have you ever been diagnosed with: High blood pressure . . . . . . . . . . . . . . . . . . . . Heart disease – angina. . . . . . . . . . . . . . . . . . - heart attack. . . . . . . . . . . . . . - irregular heart beat . . . . . . . . - heart murmur. . . . . . . . . . . . . - rheumatic heart disease . . . . - other . . . . . . . . . . . . . . . . . . . Diabetes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Lung disease – asthma. . . . . . . . . . . . . . . . . . - emphysema. . . . . . . . . . . . . . - pneumonia. . . . . . . . . . . . . . . - bronchitis. . . . . . . . . . . . . . . . Bleeding or Clotting disorder . . . . . . . . . . . . . Hepatitis. . . . . . . . . . . . . . . . . . . . . . . . . . . . . Psychiatric problems - anxiety. . . . . . . . . . . . - other. . . . . . . . . . . . . . Nervous system disease - depression . . . . . . - epilepsy . . . . . . . . - migraines . . . . . . . - other. . . . . . . . . . . Kidney disease. . . . . . . .. . . . . . . . . . . . . . . . . Gastrointestinal disease. . . . . . . . . . . . . . . . . Aids or HIV Infection. . . . . . . . . . . . . . . . . . . . Joint Replacement . . . . . . . . . . . . . . . . . . . . . Are you or Could you be pregnant . . . . . . . . . Are you taking birth control pills . . . . . . . . . . . Other medical problems . . . . . . . . . . . . . . . . . Please list Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes No No No No No No No No No No No No No No No No No No No No No No No No No No No Physician’s Name Phone Number List all medications you are taking List past surgical procedures: When was your last dental visit? Previous Dentist Name How often do you brush your teeth? How often do you floss your teeth? When was your last Full Mouth X-Ray taken? Notes: Please list other medical problems Do you smoke Yes No – If yes, how much Do you use alcohol or recreational drugs Do you regularly use aspirin Dr./Hygienist Notes: Yes Yes Yes Yes Yes Yes for how long No – If yes, how much No – If yes, how much _how often how often No No No No