TFCCedits_DJu
advertisement

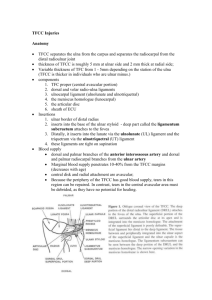
Description The triangular fibrocartilage complex [TFCC] is a soft tissue structure covering the distal ulna at the wrist, which serves to help stabilize the wrist and transmit load across the wrist joint. Because of its anatomic complexity and the forces that it experiences, the TFCC is at risk for both direct injury and degenerative damage. As such, TFCC pathology is a common cause of ulnar sided wrist pain. Structure and Function The triangular fibrocartilage complex (TFCC) is located at the ulnar wrist, articulating with the head of the ulna proximally and the lunate and triquetrum distally. Figure or MRI showing normal TFCC in situ CAPTION: The TFCC is comprised of the following: (1) the triangular fibrocartilage proper – articular disc; (2) the ulnocarpal meniscus homologue; (3) the dorsal and vo lar radioulnar ligaments; (4) the floor of the extensor carpi ulnaris (ECU) tendon sheath; and (5) the volar ulnocarpal ligaments. (Figures 1 and 2) The TFCC can be divided logically into three components. The first component of the TFCC is the triangular fibrocartilage disc itself. This disc accepts and distributes loads to the ulna from the carpus, much like the way the meniscus of the knee accepts and distributes force from the femur. Without a TFCC, the force from the carpus that the ulna is able to receive is halved, a deficit that is compensated by even greater load placed on the radius. The second component of the TFCC comprise of the radio-ulnar ligaments, which are the primary stabilizers of the distal radioulnar joint. The third and final component of the TFCC is the ulnocarpal ligament complex, which prevents dorsal migration of the distal ulna relative to the lunate and triquetrum, to which it attaches. The vascular supply of the TFCC is limited to the peripheral 10-40% of the volar, ulnar, and dorsal TFCC only. The relative hypovascular nature of the central portion of the TFCC precludes healing of injury in this region, and may necessitate surgical excision of injury with no capacity for repair. Patient Presentation Acute injuries of the TFCC result from axial and torsional forces applied to the extended wrist; in short, most often from falling on an outstretched hand (FOOSH). Failure of the TFCC may be found in association with a distal radius fracture (which also comes about from force applied to the extended wrist). Patients with TFCC injuries may present with chronic complaints of ulnar-sided wrist pain. Often, symptoms are aggravated with axial loading, particularly with the wrist in extension, or torsional activities against resistance such as wringing out a washcloth or turning a screwdriver. With progression, even simple activities such as pouring from a pitcher of water may cause pain. Pain or tenderness is localized to the ulnocarpal joint and may be provoked with ulnar impaction testing, or loading through an extended wrist such as with pushing oneself up from a chair. Patients can also complain of pain in the ulnar wrist in supinated and/or pronated positions. While the majority of TFCC injuries do not involve instability of the wrist, failure of the distal radioulnar ligaments may cause instability of the distal radioulnar joint (DRUJ). This instability may cause pain and mechanical symptoms of “popping” or subtle signs of “giving way”. There may be visible signs of instability with prominence of the ulnar head relative to the distal radius – often, it is useful to compare the appearance of both the injured and non-injured wrists for evidence of asymmetry. clinical of photo of surface anatomy for palpating TFCC Gross instability of the DRUJ may be recognized with stress testing of the DRUJ in positions of maximal pronation and supination. clinical of photo of examination TFCC DRUJ stress testing Clinical Evidence For patients with a suspected TFCC injury, advanced imaging studies may be useful in assessment of the ulnar wrist. Plain radiographs can show the congruity of the DRUJ and allow measurement of the ulnar variance. (see “risk factors”, below) xray showing positive ulnar variance Arthrography, or, better still, an MRI (or MR-arthrogram) may help detect ulnar wrist pathology. The sensitivity and specificity for detecting a full-thickness TFCC tear are approximately 85% and 95%, respectively, for MR-arthrography. The gold standard for assessing the integrity of the TFCC is arthroscopy, though this is not only an invasive test, it is one that requires anesthesia. Injuries of the TFCC can be classified as Palmer Type 1, traumatic, and Type 2, degenerative. Traumatic lesions may be further sub-classified by their location. Epidemiology Attritional tears or degenerative pathology involving the TFCC are common, with a reported incidence of tears in greater than 50% of those over the age of 60 years. (Such chronic alterations in TFCC may become symptomatic after minor wrist trauma. On the other hand, the high prevalence of asymptomatic morphological change within the TFCC makes it unwise to necessarily attribute ulnar-sided wrist pain to a structural abnormality seen on an imaging study.) It is estimated that TFCC injury occurs in up to 80% of displaced distal radius fractures. Differential Diagnosis It is important to determine whether the symptoms are intrinsic to the wrist, or whether they might be referred to the wrist from other structures. Intrinsic causes of ulnar wrist pain which might mimic symptoms associated with a TFCC include: Arthritis DRUJ ulnocarpal joint pisotriquetral joint Chondral injury (eg, acute, ulnar impaction) Fracture: hook of hamate pisiform distal radius distal ulna triquetrum Ganglion cyst, Kienbock’s disease (avascular necrosis of the lunate) Inter-carpal ligament injury ECU tendonitis/pathology Extrinisic causes include cervical radiculopathy, ulnar neuropathy at the elbow, tendinopathy of either the extensor or flexor carpi ulnaris. Rarely, a nerve tumor (schwannoma) or ulnar artery thrombosis is the cause. The correct inference from the extensive lists above is that TFCC pathology overlaps with many other conditions and therefore may be blamed when other conditions are responsible, and likewise, may be cited as the culprit when the true source of symptoms lies elsewhere. Red flags Acute traumatic injury to the wrist requires a full evaluation, including the elbow; chronic ulnar sided wrist pain does have any “red flags” per se Treatment options and outcomes Management of TFCC pathology should be guided primarily by the severity of symptoms. Other important considerations include the acuity and the location of the injury, and the response to initial treatment. Most injuries of the TFCC may be treated non-operatively: activity modification, immobilization, and analgesics are first lines of care. Immobilization is typically done above the elbow with limitation of pronation/supination of the wrist, i.e. long arm removable splint or Munster cast. For persistent symptoms, corticosteroid injection of the ulnocarpal joint or therapeutic modalities may be considered. The potential and indications for TFCC repair are influenced by the vascular anatomy of the TFCC. Acute or sub-acute injuries to the peripheral TFCC may be amenable to arthroscopic debridement and repair (arthroscopic +/- limited open repair), whereas central TFCC injuries may be treated with arthroscopic debridement when conservative management has failed to relieve symptoms. Occasionally, when arthroscopic debridement does not provide adequate resolution of symptoms, an ulnar shortening osteotomy (to create negative ulnar variance and in turn decreased ulnar load) may be needed. In cases with persistent pain and disability despite appropriate treatment to date, various salvage procedures may be considered such as joint stabilization, joint unloading or decompression, distal ulna resection, arthrodesis, and arthroplasty. In a case series report of “56 patients with triangular fibrocartilage injury (33 patients ….[no] instability of the distal radioulnar joint) , open repair of the peripheral tear produced 11 excellent, 15 good, 6 fair, and 1 poor result. Repair of peripheral tears restored functional integrity to the triangular fibrocartilage, and good to excellent results are reported in 26 of the patients treated.”(J Hand Surg Am. 1994 Jan;19(1):14354.Triangular fibrocartilage tears.Cooney WP, Linscheid RL, Dobyns JH). Among 28 patients with TFCC tears, debrided (and not repaired) one study reported excellent results in 13, good in 8, fair in 2, and poor in 5; from that the authors concluded that arthroscopic debridement of TFCC tears is “warranted”. (Arthroscopy. 1998 Jul-Aug;14(5):479-83. Wrist arthroscopy for the treatment of ligament and triangular fibrocartilage complex injuries. Westkaemper JG, Mitsionis G, Giannakopoulos PN, Sotereanos DG.) Risk factors and prevention Ulnar variance describes the relative position of the distal articular surfaces of the radius and ulna. “Positive” variance referring to the setting in which the ulna projects more distally. The significance of positive ulnar variance is that the distal ulna and TFCC are subjected to greater loading. Hence, positive ulnar variance is a risk factor for TFCC injury. (by contrast, negative variance loads the radio-carpal joint more, and in turn is a risk factor for avascular necrosis of the lunate (Kienbock’s disease ) Miscellany The term “conservative treatment” should not be used synonymously with “non-operative treatment”. There is nothing conservative about deferring surgery for a repairable TFCC tear, especially when such a delay facilitates the transformation of that repairable tear into an irreparable tear. Some people similarly refer to the “TFCC complex”. This is an instance of the “RAS Syndrome”, a (selfreferential) acronym for the Redundant Acronym Syndrome syndrome in which the word denoted by the last letter of an acronym is repeated unnecessarily. Other examples include “ATM machine” or “HIV virus”. Key Terms TFCC, triangular fibrocartilage complex, ulnocarpal joint, ulnar wrist Skills Create a differential diagnosis of ulnar sided wrist pain and perform a physical examination to hone the list.