Coronary Stents. - MyWeb at WIT - Wentworth Institute of Technology
advertisement

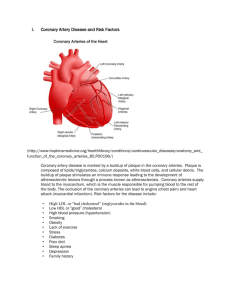
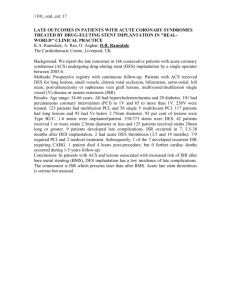
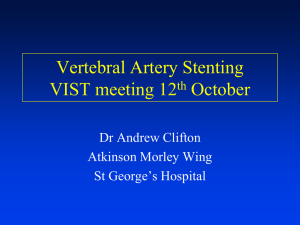
Coronary Stent Huma Abdul Rauf Maria Gonzalez BMED 101-04, Fall 2011 Wentworth Institute of Technology Dr. Douglas Dow Dr. Shankar Krishnan Abdul Rauf and Gonzalez BMED 101-04 Table of Content Introduction……………………………………………………………………………………..3 Objective ………………………………………………………………………………....…. 4-5 Background History ………………………………………………………………………….5-6 Principles …………………………………………………………………………….………6-8 Current Application/ Future Work ……………………………………………………….....8-11 Conclusion…………………………………………………………………………………….12 P age | 2 Abdul Rauf and Gonzalez BMED 101-04 Introduction Over decades, technology has evolved drastically and knowledge in science has increased rapidly. Thus, when technology has increased rapidly many questions has been answered prior to health problems and cures for disease. Atherosclerosis which is known as blockage or hardening of arteries, has been around for decades and increased the risk of heart attack, stroke and angina. Cardiovascular disease is the number one leading cause of death in United States. Majority of these cardiovascular diseases are caused by atherosclerosis also coronary arteries disease. Therefore, the discovery of coronary stents has decreased rate of deaths that are caused by cardiovascular diseases. P age | 3 Abdul Rauf and Gonzalez BMED 101-04 Objective The objective of the following research project is to overview the effects of stents and benefits on society. This project mainly focuses on coronary arteries and how they have evolved over time and the future work that is being researched. Atherosclerosis and Coronary Stent Atherosclerotic Peripheral Vascular Disease, hardening of arteries, which primarily affects the arteries. Atherosclerosis can affect any party of the body. Atherosclerosis of coronary arteries is generally limited to the large superficial epicardial vessels before they give off branches that bring blood to the heart muscle. Developed atherosclerotic plaques consist of a central core of lipid and cholesterol crystals and cells such as macrophages, smooth muscle cells and foam cells along with necrotic debris, proteins and collapsing blood elements. This central core is separated from the lumen by a fibrous cap in collagen. The major complications of atherosclerosis result from progressive obstruction of a vascular lumen, disruption of a plaque followed by thrombus formation and also destruction of the primary vascular wall. Figure 1: Atherosclerosis is caused by buildup of plaques in the walls of arteries. People with high level cholesterol and are obese are at high risk and higher chance of getting coronary disease. The most important complication is myocardial infarction, which is permanent injury to heart muscle initiated by complete thrombotic occlusion following rupture of an atherosclerotic plaque that previously was only partially obstructive. The natural history of athermanous plaque and the effectiveness and safety of interventional therapies depend in part on relative plaque composition, the spatial distribution of the constituents and the integrity of the fibrous cap, which P age | 4 Abdul Rauf and Gonzalez BMED 101-04 largely determines plaque stability. Risk factors for atherosclerosis and coronary artery disease include diabetes, systemic arterial hypertension, high levels of cholesterol, and smoking. Angioplasty is used in patients with stable angina, unstable angina, or acute myocardial infarction to restore blood flow through a diseased portion of the coronary circulation obstructed by atherosclerotic plaque and thrombotic deposits. A deflated balloon is passed over a guide wire to a site of stenosis, where the balloon is inflated using progressive and substantial expansible force. Enlargement of the lumen and increased blood flow occurs by plaque reduction through compression or rearrangement of the plaque contents and by overall mechanical expansion of the vessel wall. Figure 2: Procedure of angioplasty and a stent is inserted to keep the arteries open. http://www.youtube.com/watch?v=3Srimon14CY&feature=related Background History In 1964, Charles Theodore dotter and Melvin P. Judkings described the first angioplasty. And in 1974, Andreas Gruentzig tested using balloons on animals to test the procedure to open an artery. Angioplasty was a innovative treatment that led to the beginning of a great advanced in the cardiovascular field of medicine. Since the beginnings of stents and angioplasty many discoveries has been developed and like mentioned later great plans are in the table for the future of stent and angioplasty procedure. Today angioplasty is the most frequently performed medical procedures in clinical practice today. Coronary stents used in angioplasty where first develop in the 1980’s. and approved by the FDA in the USA in the mid 1990’s their placement is made through a balloon angioplasty to P age | 5 Abdul Rauf and Gonzalez BMED 101-04 treat coronary artery blockages. After balloon angioplasty reduces the narrowing of the artery stent is placed immediately leaving a residual stenosis of 10% or less of the original stenosis of the artery. In addition to treating coronary artery stents are used during angioplasty of any other arteries of the body, for example, is commonly used in kidney arteries, arteries of the lower limbs mainly in the iliac and has now been demonstrated effectiveness and safety of angioplasty for the treatment of blockages of the carotid arteries. This Coronary angioplasty improves the circulation to provide important benefits to society like lower chest pain, decreased the possibilities for stroke , heart attacks and decrease pain in leg arteries. Stents are not all alike, come with different textures, plasticity, elasticity, radial strength, diameter and other properties. Stents are essentially permanent devices become a part of the cardiovascular system. Stents have the risk of two long-term complications. First there is the possibility of recurrence in narrowing it at the site of stent placement (restenosis), the risk of restenosis is approximately 20% within the first 6 months of opposing the risk placed 30 - 40 restenosis following made only to Balloon Angioplasty. coronary artery: insertion of a stent into a coronary artery. Photograph.Encyclopædia Britannica Online. Principles Stents were first developed in the 1980s to address the problems and side effects of balloon angioplasty. Most patients who received balloon angioplasty would have a case of restenosis. Thus, most patients who undergo angioplasty also receive stents. Stents are expandable tubes of metallic wire and were designed to be flexible. Stents preserve luminal P age | 6 Abdul Rauf and Gonzalez BMED 101-04 patency and provide a larger and more regular lumen by acting as a support to the disrupted vascular wall. Stents were also introduced to minimize thrombus formation following angioplasty and thereby reduce the impact of post angioplasty restenosis. Stent technologies have rapidly increased. The majority of stents in use today are composed of balloon expandable 316L stainless steel or nitinol mesh tubes that range from 8 to 38 mm and from 2.5 to 4.0 mm in diameter. Current stents that are in use today are follows: Cordis Palmaz-Schatz stent, the Cordis Crossflex stent and Medtronic stent. Development has focused on permitting stents to become more flexible and more easily delivered and deployed. The choice of stent is based on several factors, including the characteristics of a given plaque, such as its diameter, length, and location within the coronary structure, and the experience of the interventional cardiologist with a particular stent. Figure 3: The size of a stent relative to the hand. P age | 7 Abdul Rauf and Gonzalez BMED 101-04 Figure 4: Stents have been are special designed such as having wider peaks, shorter segments and nested peaks that avoid contact with each other which helps keep the arteries open. Thus, stents are mainly composed of metal alloys or compound materials which vary in shapes and sizes depending on the manufacturer and the organ that is being placed in. Current Application/ Future Work Every day more and more solutions are being research to solve the future problems derivate from the implantation of coronary stents. Improvements have been happening from the 90’s purely mechanical improvements but to pharm logics points of views. Drug- Eluting Stents Current research project are being held on stents that prevent restenosis, one of the main discoveries so far is the idea of finding drugs that inhibit biological processes that causes restenosis. The stent are coated with these drugs, sometimes wrapped in a layer thin of thin polymer that retards their action. From the year 2002 two systems were found that have had good results in this field. An immunosuppressive drug called Sirolimus manufactured by Wyeth-Ayerst, which Johnson and Johnson and Cordis have used before in the past to cover their stent CYPHER. The results after 8 months of testing were very positive, was reduction in presence of restenosis raging between 3.2 and 91%. Today in 2012 CYPHER is considered the first of an advanced generation of hearth Stents Called drug coated or “drug eluting” stents. Cypher has been used to open blocked arteries for more than 3 million people. The CYPHER stent has been evaluated in more than 45,000 people in over 75 clinical studies. P age | 8 Abdul Rauf and Gonzalez BMED 101-04 The second System that has had great results like cypher is the research done for 6 months at the Boston Scientific TAXUS II. TaxusII is a research based on a stent by Boston scientific. The research consisted on using the stent and covered it with a polymer that delivers the paclitaxel drug fabricated in Canada by a company named Angiotech. Pactixel is a principle find in a drug called TAxol. Paclixatel has been used in the passed Currently in the market DES (Drug-eluting stents) has two models that have been approved by the FDA (Food Administration) each stents is about $2500 a piece but also many stents are in current medical in medical trial. The approved stents are made of 316L of stainless steel with a polymer containing a specific drug to prevent restenosis. The polymers control the rate which with the medicine goes into the body. Stents treated with ionic Implementation Another technique applied to treat the surface of cardiovascular stents is the ion implantation. The ions penetrate to an area near the surface, this process does not form any new layer so that no problems adhesiveness. Using this technique it is possible to enrich the surface up to 91% of foreign ions so if you make a good choice of these can be clearly improve the biocompatibility of the material. The introduction of C and ion strange displaces nickel into the substrate. In addition, the depth of penetration of ions is low (about 20Mn) so are not altered mechanical properties of the substrate material P age | 9 Abdul Rauf and Gonzalez BMED 101-04 Stents with Radiation. Stent with radiation is another technique that is being investigated which includes the use radioactivity as a measure to prevent the occurrence of restenosis in patients. Patents have been written in which the application of this technique and the introduction of drugs are key to a good patients responses to the cardiovascular stent placement. The invention consists in a coating containing a radiation source emitting β or γ radiating to the tissues and prevents the proliferation of cells in the wound response in angioplasty. This coating has a second layer deposited on top substance containing anticoagulant that radiation never is in direct contact with the patient’s body. All these new techniques involving the superposition of layers with different focus functions all research in this field since the main goal is find the combination of techniques able to eliminate the problem of training clotting and restenosis. P age | 10 Abdul Rauf and Gonzalez BMED 101-04 Porous stents introduction of drugs Another method being investigated to improve the problem of restenosis is manufacture of porous stents. As shown in the figure layouts can be varied as needed. In the figure a) can be seen that the size of pores is higher inside than outside. This provides high capacity drug storage inside and a much lower expulsion rate. This treatment may last longer. In the case of Figure b) there are two parts separated by a central solid. Both the top and bottom are porous so that you can enter drugs. Moreover, since there are communicated with each other can be introduced different drugs. These are specific to the area to be in touch with the material, the wall of the vein or blood. There are many other combinations in other cases you can do playing with pore size distribution. For its versatility this is a line of research that is taking a lot of strength. P age | 11 Abdul Rauf and Gonzalez BMED 101-04 Conclusion The use of cardiovascular stents has been a great advance in medicine and biomedical engineering. Stents have helped to the lower risk for humans to suffer from severe cardiac disease. The risk of Restenosis has been highly reduced in a 33% with respect to the process of traditional angioplasty. Currently in the market the presence of various Biomedical Engineering companies have permitted that we can have more than 100 different types of stents being fabricated. This has permitted doctors around the world to have more options when choosing the right stent for different patients. On the other hand, the great advances in the drug-eluting stents are currently being every day more and more successful showing a bright future for stent technology. The risk for restenosis is less and less day by day by combining different drugs depending on the condition of the patient. Different investigations have been made about the surface of treating stents like the ionic implementation to eliminate the contact of the body with the damaging ions like Ni. During this research another idea has been brought to the table. The project consists in coloring the stainless steel creating a barrier with the ions enabling researchers to evaluate the behavior of the ions with the blood. This method of coloration is a cheaper solution for stent technology and would be a huge impact on stent price. P age | 12 Abdul Rauf and Gonzalez BMED 101-04 References: (1)Garg, Scot, and Patrick W. Serruys. "Coronary Stents." Journal of the American College of Cardiology 56.10 (2010): S1-S42. Health Reference Center Academic. Web. 7 Dec. 2011. (2) RATNER, BUDDY D. Biomaterials Science. An introduction to materials in medicine. San Diego, California: 1996, p. (3) MICHAELS, ANDREW D.; CHATTERJEE, KANU. Angioplasty versus Bypass surgery for coronary disease. Cardiology Patient Page. 2002. Vol. 106, p.187-190. http://www.circulationaha.org (4) "Stent Review - Cath Tech.com." Home - Cath Tech.com. Web. 07 Dec. 2011. http://www.cathtech.com/content/view/17/1/ (5) Ratner, Buddy D.; Hoffman, Allan S.; Schoen, Frederick J.; Lemons, Jack E. (2004). Biomaterials Science - An Introduction to Materials in Medicine (2nd Edition).. Elsevier. Online version available at: http://www.knovel.com/web/portal/browse/display?_EXT_KNOVEL_DISPLAY_bookid=3002 &VerticalID=0 (6)Hacker, Andrew, and Claudia Dreifus. "Are Colleges Worth the Price of Admission? Commentary - The Chronicle of Higher Education." Home - The Chronicle of Higher Education. Web. 05 Dec. 2011. <http://chronicle.com/article/Are-Colleges-Worth-the-Price/66234>.) (7) Lim, Issel Anne. Biocompatibilty. MIT. Web. <http://web.mit.edu/murj/www/v11/v11Features/v11-f5.pdf>. P age | 13