Poisoning and Overdose
advertisement

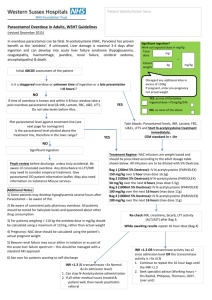
Poisoning and Overdose Section A- choose the correct drug 1. A 25 year old is rushed to A&E presenting with confusion and temperature of 38.9oC. Her blood pressure is fluctuating and she has a markedly raised creatinine phosphokinase. 2. A man says that his depressed partner has taken an overdose. She is drowsy and hypotensive with signs of respiratory depression. There is no response to naloxone. Drugs Captopril Amitriptyline Atenolol Paracetamol Ecstasy Heroin Diazepam Cocaine Risperidone 3. A 40-year-old depressed man is brought to A&E with dilated pupils, blurred vision and seizures. On examination he is tachycardic and his ECG shows wide QRS complexes. 4. A 35-year-old intravenous drug user (IVDU) presents comatose with pin-point pupils and respiratory depression. Section B- choose the correct treatment 5. A 40-year-old drowsy woman is brought to A&E with headache and vomiting with flushed cherry-pink skin. Carboxyhaemoglobin (COHb) is 40 per cent. 6. A 20-year-old woman presents to A&E with confusion, sweating and blurred vision after taking some ecstasy. She has a rectal temperature of 40.5°C. Creatine kinase is 4000 U/l. Treatment Desferrioxamine N-acetylcysteine Naloxone Oxygen Atropine Atenolol IV fluids Vitamin K Metoclopramide + paracetmol 7. A 32-year-old woman presents 6 hours after a paracetamol overdose. The paracetamol level is above the treatment line. 8. A 7-year-old boy presents to A&E with constricted pupils, sweating and increased salivation after drinking a bottle of insecticide lying in the garden. Common Toxidromes Toxidromes Anticholinergic Cholinergic (muscarinic) Sedative/Hypnotic Drugs involved Antihistamines, tricyclic antidepressants (amitriptyline), atropine Organophosphates (nerve gases, insecticides), Carbamates (insecticides) Benzodiazepines, barbiturates, alcohols, opioids (heroin), anticonvulsants, antipsychotics Sympathomimetic Salbutamol, amphetamines, MDMA, cocaine, Serotonin syndrome Commonly with combinations of drugs that affect serotonin reuptake: MAOi + any other antidepressant Antidepressant + pethidine/tramadol Antidepressant + MDMA/LSD Any antipsychotic Neuroleptic malignant syndrome Withdrawal Principles of management Presentation Tachycardia, hyperthermia, mydriasis, warm and dry skin, urinary retention, ileus, delirium SLUDGE syndrome (salivation, lacrimation, urination, defecation, GI cramps, and emesis), miosis, bronchorrhea, wheezing, bradycardia Sedation, hypoventilation, hypotension Opioids + barbiturates also cause: miosis, possibly hypothermia Tachycardia, hypertension, mydriasis, agitation, seizures, diaphoresis, hyperthermia, psychosis (after chronic use) Common: Diarrhoea, sweating, ataxia, tremor, disorientation, hypomania Distinguishing: Myoclonus, hyperreflexia Extreme pyrexia, stiffness, confusion, autonomic instability (BP and pulse up and down), raised WBC, raised creatinine phosphokinase ++++ Tachycardia, hypertension, mydriasis, diaphoresis, agitation, restlessness, seizures, hyperreflexia, piloerection, yawning, abdominal cramps, lacrimation, hallucinations Drug Paracetamol Opioid Iron Carbon monoxide Ethylene glycol/methanol Digoxin Cholinergics Antidote N-acetylcysteine Naloxone Desferrioximine Oxygen Ethanol/fomepizole Full history including: o HPC: Quantity and route Timing Staggered? Patient’s own medication or other Digoxin antibodies source Atropine Coingestions Symptoms/events following ingestion Collateral history o Assessment of suicidal risk o Past psychiatric history Refer to TOXBASE For most poisonings, treatment is symptomatic and supportive care Gastric decontamination if recommended (e.g. gastric lavage, oral activated charcoal) Antidotes (relatively few) Enhanced elimination if recommended (e.g. haemodialysis, haemofiltration, charcoal haemoperfusion