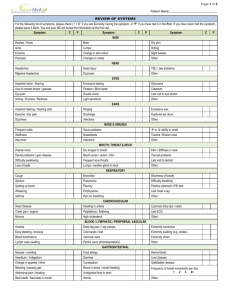
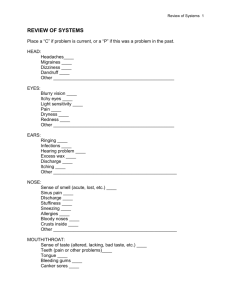
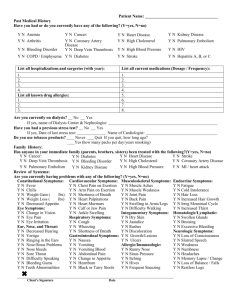
Review of Systems Form
advertisement

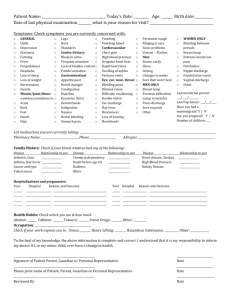
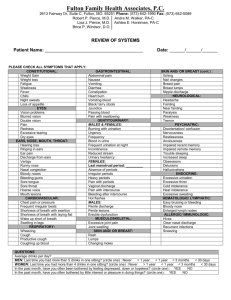
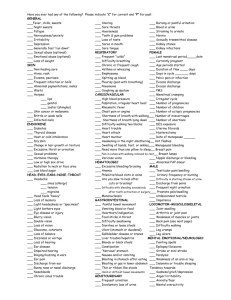
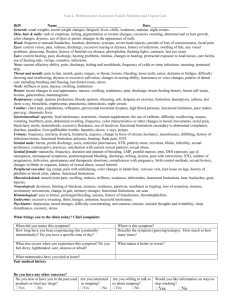
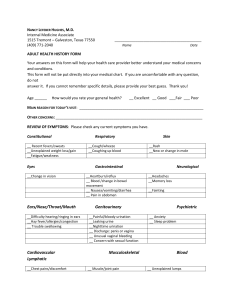
NAME:___________________________________ DOB:___/___/___ TODAY’S DATE:___/___/___ IF female is there any chance that you might be pregnant? YES or NO Date of LMP___/___/___ or N/A Please list the medications you are currently taking, their dosages, and how many times per day you take them: _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ Do you have any ALLERGIES or intolerances to drugs, latex, food, insects, etc? YES or NO If YES, provide a description of each allergy including the type of reaction: _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ Medical History: _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ Family History: _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ Do you use Tobacco? __________ Do you smoke? __________ How many a day? __________ How many years? __________ Have you attempted to quit? __________ Do you drink? __________ How often (please circle)? Social Occasional What do you drink (please circle)? Beer Wine Liquor Light Heavy Surgical history: _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ Immunization History (Please include dates): _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ Reason for today’s visit: _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ Constitutional: Chills? Decline in Health? Fatigue? Fever? Head: Dizziness? Fainting? Headaches? Eyes: Discharge? Excessive tearing? Redness? Vision loss? Eye pain? Infections? Recent injury? Pain? Which ear? Ringing in ears? Nose: Discharge? Nasal obstruction? Nosebleeds? Ears: Discharge? Hearing aid? Hearing impairment? Mouth: Bleeding gums? Postnasal drip? Tongue burning? Voice changes? Lumps? Tenderness? Tonsils enlarged? Wheezing? Short of breath? Is cough productive? Chest pain? Palpitations? Varicose veins? Leg pain-walking? Short of breathexertion? Short of breathlying flat? Short of breathsleeping? Swelling of legs? Abdominal pain? Constipation? Diarrhea? Heartburn? Rectal bleeding? Change in stool consistency? Decreased appetite? Hemorrhoids? Nausea? Rectal pain? Swallowing problems? Vomiting? Vomiting blood? Joint pain? Back problems? Joint stiffness? Muscle cramps? Muscle stiffness? Restricted motion? Weakness? Throat/Neck: Frequent sore throat? Respiratory: Cough? Cardiovascular: Gastrointestinal: Musculoskeletal: Psychiatric: Depression? Behavioral changes? Disturbing thoughts? Excessive stress? Hallucinations? Memory loss? Mood changes? Nervousness? Lumps? Pain? Tenderness? Dryness? Hair texture change? Hives? Mole increased size? Dizziness? Headaches? Memory loss? Numbness? Weight loss? Increased thirst? Cold intolerance? Sweats? Excessive urination? Fatigue? Bleeding easily? Easy bruisability? Lumps? Swollen glands? Coughing? Hives? Itchy eyes? Itchy nose? Recurrent infections? Runny nose? Sneezing? Stuffy nose? Watery eyes? Breast: Discharge? Skin: Itching? Neurological: Loss of consciousness? Unsteady gait? Endocrine: Weight gain? Heat intolerance? Hematologic/Lymph: Anemia? Allergic/Immunologic? Urinary: Awakening to urinate? Incontinence? Blood in urine? Burning? Excessive urination? Frequency? Infections? Pain on urination? Urgency? Hernias? Sexual problems? Lesions? Venereal disease? Pain? Prostate problems? Bleeding between periods? Change in periodsduration? Change in periodflow? Change in periodsinterval? Discharge? Itching? Lesions? Menstrual pain? Pain on intercourse? Postmenopausal bleeding? Male genitalia: Discharge? Scrotal masses? Female genitalia: Sexual problems?