Supplemental Content
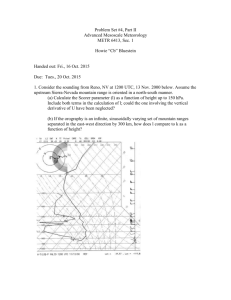
advertisement

Electronic supplement Methods Study device The Absorb BVS consists of a polymer backbone of Poly-L lactide (PLLA) coated with a thin layer of a 1:1 mixture of Poly-D, L-lactide (PDLLA) polymer, and the anti-proliferative drug everolimus to form an amorphous drug eluting coating matrix containing 100 micrograms of everolimus/cm2 of scaffold. The details of the device have been previously described (1,2). The scaffold design has in-phase zigzag hoops linked by bridges that allow a uniform strut distribution and provide uniform vessel wall support and drug transfer. Study Procedure Target lesions were scaffolded after mandatory pre-dilatation. Post-dilatation with a balloon shorter than the implanted scaffold could be performed at the operator’s discretion (if an optimal angiographic result was not obtained immediately after scaffold deployment). Additional stenting with a Xience V drug-eluting metallic stent for edge dissection or insufficient coverage of the lesion occurred in 3 out of the 101 patients. Treatment with aspirin was started at least 6 hours prior to the index procedure (3). A loading dose of 300 mg of clopidogrel was administered before the procedure, followed by 75 mg daily for a minimum of 6 months. 3-Dimensional OCT To visualize more comprehensively in three dimensions, connections and disconnections of the struts inside the global structure of the scaffold, 3-D OCT analysis was used (2,4). First, image sequences were generated from the OCT image files. Every single strut was detected in each OCT cross section. After segmentation of scaffold struts, three-dimensional images were reconstructed using a volume rendering software (OSIRIX, version 3.8.1). X and Y axis pixel resolution were calculated in each image sequence using the image software (Image J), while the slice interval was set as 0.2 mm, according to the pullback speed of 2.0 mm/s and the frame rate of 100 frame/second. To display the changes in spatial distribution of the struts along the scaffold from post-procedure to late follow-up, the ‘spread-out-vessel chart’ was used as described previously (5). Briefly, these graphics were obtained by correlating the longitudinal distance from the distal edge of the scaffold to the strut (abscissa) with the angle where the struts were located in the circular cross section with respect to the center of gravity of the vessel (ordinates). In each cross-section (axial resolution of 200 microns), the circumferential length of each individual strut was depicted in an angular fashion. The resultant graphic represented the scaffolded vessel, as if it had been cut longitudinally along the reference angle and spread out on a flat surface. IVUS greyscale analysis Treated vessels post-procedure and at follow-up were examined with phased array intravascular ultrasound catheters (EagleEye™; Volcano Corporation, Rancho Cordova, CA) using a pullback speed of 0.5 mm per second (6). The presence of scaffold disruption was assessed using the same criteria used in OCT analysis. 1 Definitions The composite ischemia-driven major adverse cardiac event (ID-MACE) was cardiac death, any myocardial infarction and ischemia driven TLR for a QCA diameter stenosis (DS) of ≥50% with either symptoms or ischemia, or DS ≥70% at the time of scheduled or unscheduled angiography. For non-Q MI, elevation of CK levels ≥2 times the upper limit of normal with elevated CK-MB was required, a definition dating from the design time in 2008 (7). All events were adjudicated by an independent clinical event committee and all imaging procedures (QCA, IVUS Grayscale, IVUS-VH, echogenicity and OCT) were analyzed by an independent core lab (Cardialysis B.V., Rotterdam, the Netherlands). 2 Table e1. Baseline characteristics p values Total Cohort B1 Cohort B2 51 patients 30 patients 21 patients 52 lesions 30 lesions 22 lesions Age (mean ± SD, years) 62 ± 10 64 ± 10 59 ± 9 0.1 Male gender (n (%)) 37(73) 22(76) 15(68) 0.75 Current Smokers (n (%)) 12(24) 5(17) 7(32) 0.32 4(8) 3(10) 1(5) 0.63 Hypertension Requiring Medication (n (%)) 30(59) 16(55) 14(64) 0.58 Hyperlipidemia Requiring Medication (n (%)) 38(75) 26(90) 12(55) 0.01 Prior target vessel Intervention (n (%)) 11(22) 8(28) 3(14) 0.31 Prior myocardial infarction (n (%)) 15(29) 12(41) 3(14) 0.06 Left Anterior Descending (n(%)) 27(53) 13(45) 14(64) 0.26 Left Circumflex (n(%)) 9(18) 7(24) 2(9) 0.27 Right Coronary Artery (n(%)) 16(31) 10(35) 6(27) 0.76 A (n(%)) 0 0 0 - B1 (n(%)) 28(57) 15 (52) 13 (65) 0.39 B2 (n(%)) 20(41) 13(45) 7(35) 0.56 C (n(%)) 1(2) 1(3) 0 1 Mean Reference Vessel Diameter (mm) 2.61 ± 0.33 2.63 ± 0.37 2.57 ± 0.27 0.52 Minimum Luminal Diameter (mm) 1.08 ± 0.27 1.06 ± 0.29 1.12 ± 0.25 0.43 B1 vs. B2 Diabetes (n (%)) Target Vessel AHA / ACC Lesion Classification 3 58 ± 11 59 ± 11 56 ± 10 0.34 Lesion Length (mm) 10.1 ± 3.6 10.7 ± 4.0 9.2 ± 2.7 0.15 Maximum diameter of balloon at scaffolding or post-dilatation 3.03 ± 0.24 3.08 ± 0.23 2.96 ± 0.24 0.1 Mean diameter of balloon at scaffolding or post-dilatation 2.55 ± 0.27 2.78 ± 0.21 2.69 ± 0.22 0.14 29 (57) 15(52) 14(64) 0.57 Diameter Stenosis (%) Post dilatation (n(%)) 4 Table e2. Patient and lesion characteristics in patients with or without late discontinuities Cases with late discontinuities 21 patients 21 lesions Cases without late discontinuities 28 patients 29 lesions 63.7 ± 11.2 15 (71.4) 5 (23.8) 2 (9.5) 60.7 ± 0.16 21 (72.4) 6 (20.7) 1 (3.4) 0.29 1 1 0.57 Hypertension Requiring Medication (n (%)) 11 (52.4) 19 (65.5) 0.39 Hyperlipidemia Requiring Medication (n (%)) 13 (61.9) 4 (19.0) 8 (38.1) 24 (82.8) 7 (24.1) 6 (20.7) 0.12 0.74 0.3 9 (42.9) 4 (19.0) 8 (38.1) 17 (58.6) 5 (17.2) 7 (24.1) 0.39 1 0.36 0 10 (50) 9 (45.0) 1 (5.0) 2 (10.0) 0 17 (60.7) 11 (39.3) 0 (0) 7 (25.0) 0.56 0.77 0.42 0.27 2.59 ± 0.37 1.21 ± 0.30 53.4 ± 10.2 10.0 ± 3.86 0.05 ± 0.05 2.62 ± 0.31 1.00 ± 0.22 61.2 ± 10.2 10.2 ± 3.49 0.04 ± 0.04 0.77 0.01 0.01 0.91 0.33 14 (66.7) 14 (48.3) 0.25 2.83 ± 0.36 2.87 ± 0.27 0.69 2.56 ± 0.30 2.56 ± 0.24 0.99 0.18 ± 0.18 0.18 ± 0.16 0.96 Age (mean ± SD, years) Male gender (n (%)) Current Smokers (n (%)) Diabetes (n (%)) Prior coronary Intervention (n (%)) Prior myocardial infarction (n (%)) Target Vessel Left Anterior Descending (n(%)) Left Circumflex (n(%)) Right Coronary Artery (n(%)) AHA / ACC Lesion Classification A (n(%)) B1 (n(%)) B2 (n(%)) C (n(%)) Calcification (n(%)) Preprocedure Reference Vessel Diameter (mm) Minimum Luminal Diameter (mm) Diameter Stenosis (%) Lesion Length (mm) Curvature before scaffolding (cm-1) Post dilatation (n(%)) Maximum diameter of balloon after scaffolding or post-dilatation (mm) Mean diameter of balloon after scaffolding or post-dilatation (mm) Absolute recoil (mm) P values 5 Figure e1. Flow chart of patient with OCT at baselines and follow-up BL= baseline, 6M = 6 months, 24M = 24 months, 36M = 36 months, OCT = optical coherence tomography 6 Figure e2 Each series of framed illustrations (yellow, green and orange) represents the observation at different time points (post-procedure, at 6 months and at 2 years). An Absorb BVS 3.0 mm scaffold was implanted with good conformability in an angulated stenosed segment of a RCA (A: pre-procedural angiography, B: post procedural angiography, white arrows indicate the extremities of scaffolded segment). On OCT (C-F), the scaffold was well expanded with full apposition of struts. At 6 months, the repeat angiography showed a good persistent result (G). IVUS did not show any abnormality (H), however, OCT (I-L) showed a malapposed proximal metallic marker (J, white arrow) as well as overhung struts (K, white arrows). Panels M and N shows 3-D reconstruction of OCT images at 6 months. White arrow indicates the proximal marker and malapposed overhung struts, which are connected proximally and distally to the vessel wall. At 24 months (2Y), angiography (Q) and IVUS (R) showed patency of the scaffolded segment. The malapposed proximal marker (white arrow in T) and overhung strut (white arrow in V) still remained on OCT (S-V). Although these covered struts seemed to be malapposed and overhung on 2-dimension (V), they were attached to the vessel wall on 3-dimension (white arrows in O and P). 7 Figure e3 Each series of framed illustrations (light blue, yellow and light green) represents the observation at different time points (post-procedure, at 1 year and at 2 years). The figure shows a case with non-ischemia driven TLR. An Absorb BVS 3.0 mm scaffold was implanted in the mid LAD lesion (post procedural angiography: G, white arrows indicate the scaffolded segment). Immediately after the procedure, OCT demonstrated a good expansion of the scaffold without any malapposition (B and C). Planned angiography at 1 year showed late lumen enlargement with, on OCT (E and F), malapposed and stacked struts (late discontinuity). The patient remained asymptomatic but the investigator, concerned by the malapposed struts observed at one year, performed a non-protocol mandated angiography at 2 years. Two-year angiography demonstrated a patent scaffolded segment with further angiographic lumen enlargement (G). OCT (H, I and J) and IVUS (K and L) showed malapposed struts in the scaffolded segment. Despite the absence of documented ischemia, an additional metallic stent in the previously scaffolded segment was implanted followed by post dilatation with a larger balloon. 8 References 1. 2. 3. 4. 5. 6. 7. Okamura T, Garg S, Gutiérrez-Chico J et al. In vivo evaluation of stent strut distribution patterns in the bioabsorbable everolimus-eluting device: an OCT ad hoc analysis of the revision 1.0 and revision 1.1 stent design in the ABSORB clinical trial. EuroIntervention 2010;5:932-938. Serruys PW, Onuma Y, Ormiston JA et al. Evaluation of the second generation of a bioresorbable everolimus drug-eluting vascular scaffold for treatment of de novo coronary artery stenosis: six-month clinical and imaging outcomes. Circulation 2010;122:2301-12. Smith SC, Jr., Feldman TE, Hirshfeld JW, Jr. et al. ACC/AHA/SCAI 2005 guideline update for percutaneous coronary intervention: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (ACC/AHA/SCAI Writing Committee to Update 2001 Guidelines for Percutaneous Coronary Intervention). Circulation 2006;113:e166-286. Onuma Y, Serruys PW. Bioresorbable scaffold: the advent of a new era in percutaneous coronary and peripheral revascularization? Circulation 2011;123:779-97. Gutierrez-Chico JL, Radu MD, Diletti R et al. Spatial distribution and temporal evolution of scattering centers by optical coherence tomography in the poly(L-lactide) backbone of a bioresorbable vascular scaffold. Circ J 2012;76:342-50. Mintz GS, Nissen SE, Anderson WD et al. American College of Cardiology Clinical Expert Consensus Document on Standards for Acquisition, Measurement and Reporting of Intravascular Ultrasound Studies (IVUS). A report of the American College of Cardiology Task Force on Clinical Expert Consensus Documents. J Am Coll Cardiol 2001;37:1478-92. Tunstall-Pedoe H, Kuulasmaa K, Amouyel P, Arveiler D, Rajakangas AM, Pajak A. Myocardial infarction and coronary deaths in the World Health Organization MONICA Project. Registration procedures, event rates, and case-fatality rates in 38 populations from 21 countries in four continents. Circulation 1994;90:583-612. 9