BMW19: 109893/09, 115766/09, 112373
advertisement

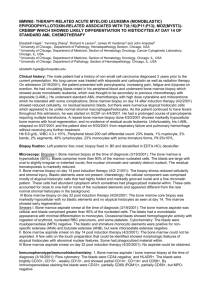
BMW19: 109893/09, 115766/09, 112373-75,09 Christine R Beham-Schmid , Sabine Hojas , Sigrun Sodia and Peter Kroisel 1.Medical University, Pathology, Graz, Austria 2.General Hospital, Division of Haematology, Fürstenfeld, Austria 3.Medical University, Human Genetics, Graz, Austria 1 2 3 3 christine.beham@medunigraz.at Clinical history: A previously healthy Caucasian 69 years old farm labourer presented with fever, night sweats, weight loss (3 kg within 2 months). At admission to the General Hospital Fürstenfeld on September 14th 2009 the patient showed bilateral leg swelling and generalized lymphadenopathy. The lymph nodes measured 4.5 cm in greatest diameter. Liver was not enlarged, there was slight splenomegaly. Due to marked leukocytosis, eosinophilia and lymph node enlargement bone marrow biopsy was performed (No: 1098934.09) and myeloproliferative neoplasm was supposed. Since no Philadelphia chromosome, BCR-ABL1 fusion gene or mutation of JAK2 could be detected, an inguinal lymph node (greatest diameter 4.5 cm) was removed on Septembert 28th and sent to the Institute of Pathology, Graz. The lymph node showed infiltration by Tlymphoblastic lymphoma and myeloid sarcoma. Thus, 8p11 myeloproliferative syndrome was assumed. The patients bone marrow biopsy was re-evaluated and a second bone marrow biopsy was performed. Due to increasing leukocytosis (69.8 G/L October 23) the patient received hydroxyurea 500mg 2 x 1. Lymph nodes were regredient, however, fever was permanently 38.5 and additional antibiotic treatment was started. Despite intensive treatment the patient died on January 9, 2010. No autopsy was performed. Hb September 14th 2009: 13.2 g/dl, September30th 2009: 14.5 g/dl, October 6th 2009: 12.5 g/dl. WBC September 14th 2009: 39.0 G/L, September 30th 2009: 23.4 G/L, October 6th 2009: 37.9 G/L, October 23th 2009: 69.8 G/L. Plt September 14th 2009: 181 G/L, September 30th 2009: 217 G/L, October 6th 2009: 172 G/L. Other lab. Parameters: Blood count (at admission): eutrophils: 67.2 %; eosinophils: 23.4 %; basophils: 0.0 %; lymphocytes: 4.4 %; promyelocytes: 4 %; myelocytes: 4 %; metamyelocytes: 5 %; segmented granulocytes: 65 %; lymphocytes: 4%; monocytes: 1.0 % LDH: 202 U/L, fibrinogen: 417.00 mg/dl (normal range 180 - 350), liver and renal parameters within normal range, no evidence for viral infections. Biopsy fixation: Bone marrow biopsy 109893/09: fixed in Carnoy solution and embedded in methylmethacrylate (semi-thin sections). Bone marrow biopsy 115766/09: fixed in buffered formalin Microscopy: Both bone marrow biopsies are highly hypercellular mainly due to increase of eosinophilic differentiated granulocytopoiesis with maturation. Left-shifted erythropoiesis is slightly to moderately increased showing occasional dysplastic changes. Polymorphic megakaryocytopopiesis is slightly increased with a few atypical forms. No fibrosis. Slightly decreased iron deposits. Immunophenotype/immunohistochemistry: CD71, glycophorin C: increased erythrocytopoiesis. CD34: endothelial cells, few megakaryocytes. CD61: megakaryocytes. EPX: eosinophils. Few B-lymphocytes (CD19, CD20, PAX5), normal T-cell population with CD2, CD3, CD4, CD5, CD8 CD56 negative. Granulocytopoiesis was stained with MPO, lysozyme, myeloid AB1, CD13, CD15, CD33, CD66, CD68. CD163: only macrophages. EBER negative. Cytogenetics: A new variant of the 8p11 myeloproliferative syndrome was identified by cytogentic and molecular cytogenetic techniques in a patient with the translocation t(1;8)(p11;q31) in his bone marrow cells. Molecular analysis: JAK2 negative. BCR-ABL negative. HemaVision negative. FLT3, NPM1 negative. Proposed diagnosis 8p11 myeloproliferative syndrome Interesting feature(s) of the submitted case 8p11 myeloproliferative syndrome is a quite rare condition. In this patient a new variant with the translocation t(1;8) (p11;q31) in the bone marrow cells could be identified. Other comments: Since it is well established that a rearrangement of the fibroblast growth factor receptor 1 (FGFR1) gene located on chromosome 8p11 with other genes at different chromosomal sites like 13q11-12 results in formation of a fusion gene with constitutively active FGFR1 tyrosine kinase activity, it appears likely that another gene located at the chromosomal breakpoint at 1q31 could be involved in the development and/or progession of this disorder.