Table 2 Probability of Falling - Springer Static Content Server
advertisement

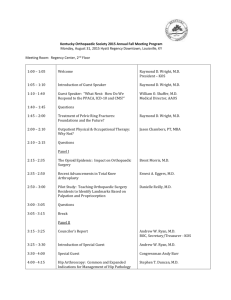
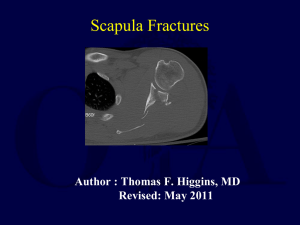
Technical Appendix Decision-analytic model A Markov model was used to model fall-related outcomes. The model contains four health states including; low risk (individuals who have never fallen), 2) medium risk (individuals who have previously fallen but incurred no injury), 3) high risk (previously injured faller) and death (due to a fall or all cause death). The decision tree imbedded within the Markov model outlines the different outcomes for older individuals. Within the decision tree the probability of transitioning to another state depends on the occurrence of various events, such as presenting at the emergency department and being admitted to hospital. At each decision node, the probability is dependent upon age as well as the risk of falling. Assumptions made in the model: Individuals who fall (fallers) have a fall rate multiplier applied to each fall to represent the fact that some people fall multiple times in one year The death rate by age is applied at each chance node to represent death from all causes. Death due to falls is also included. Those who fall and are not injured are assumed not to incur any costs Those who fall (with minor injury) and do not go to emergency incur the cost of seeking other medical attention The utility loss due to fear of falling is applied to the medium and high risk fallers at the beginning of each stage. The disutility associated with fear of falling is applied for one year only. The perspective of the cost analysis is limited to the costs incurred by the health care system due to falls Once an individual progresses to a higher risk state they cannot return to a lower risk state. For example, once a low risk faller falls and becomes injured, they then transition to being a high risk faller and remain a high risk faller for the remainder of the analysis. Model Validation The Markov model was validated using the Markov traces to compare both fall rates and death rates with population estimates. For example, based on residential aged care in Australia 2010-11 statistics, the number of residents dying within 1 year (38%) and within 5 years (82%) is equivalent to our Markov trace, in which 35% and 85% die within these time frames. As part of the model validation, a fall rate factor adjustment of 1.2 was added to take into account individuals who fall multiple times in one year. The fall rate factor was applied every time an individual falls and all resulting health care costs and utility decrements are adjusted accordingly. The costeffectiveness results are not sensitive to this adjustment. Cycle length A cycle length of one year was chosen, as the majority of the effectiveness data was for trials with an average follow-up of 12 months. Furthermore, the falls statistics (such as fall rate) are usually measured as yearly rates. A fall rate factor adjustment was used in the model to account for multiple falls in a year. Effectiveness values Literature review A systematic literature review was conducted to identify suitable studies to include in the analysis based on inclusion and exclusion criteria (see table 2 below). The searches were conducted in a number of electronic databases, with all searches conducted from 1990 onwards. Results were limited to those studies published in English, in humans and in study populations with a mean age greater than 65. Relevant final outcome measures included the number of falls and fallers or the rate of falls and fallers. Only studies with a sample size greater than or equal to 20 were included. Given that the systematic review included the same studies as the Cochrane review which was published, the results from the Cochrane review were used. Table 2 Probability of Falling Inclusion criteria Population mean age ≥ 65 years Community-dwelling or RACF residents (private homes, retirement villages, hostels, nursing homes, etc) including those attending A&E, outpatient clinics and hospital rehabilitation wards Relevant final outcome measures (falls and fallers) New fractures in subpopulations with a prior history of fractures) Australia, NZ, Canada, US, UK, Scandinavia, Japan, Taiwan, Korea and developed European countries Systematic reviews of RCTs, single RCTs, and pseudoRCTs (Level I, II, III-1 evidence, respectively, see Table 7) English full text papers Study data collected after 1990 Exclusion criteria Non relevant population (mean age < 65 years) Hospital inpatient population Non relevant intermediate outcome measures (fear of falling, falls self-efficacy, fall risk, balance, strength, mobility, etc) Non relevant and developing countries Comparative studies, with and without concurrent control groups, and case series studies (Level III-2, III-3 and IV evidence, respectively, see Appendix D) Population-based studies*, pilot studies and method studies Papers published in non-English language without an English abstract Study data collected prior to 1990 Trial participants, N < 20 Vitamin D supplementations The effectiveness of Vitamin D supplementation used in the model differed from the Cochrane review (analysis 4.1). This is because the Cochrane review included a study by Grieger 2009(1) which used a multi-vitamin containing low dose vitamin D. Figure 1 below demonstrates the results excluding the Grieger 2009 study from the analysis. The resulting rate ratio is 0.72 (0.55, 0.95), demonstrating that Vitamin D supplementation significantly reduced the rate of falls compared to no vitamin D supplementation. The four trials included in the analysis were all conducted in older people at residential aged care facilities with mean ages ranging from 83 to 89 years. The intervention used in the costing included 1,000 UI of Vitamin D and 600 mg of calcium based on the supplementation included in the trials. Bischoff 2003(2) and Broe 2007(3) supplemented patients with 800 UI of Vitamin D, Flicker 2005(4) used 1000 UI of Vitamin D and Law 2006 used 1,100 UI of Vitamin D. Figure 1. Comparison of Vitamin D supplementation compared to no Vitamin D supplementation. Medication Review The effectiveness of Medication Review was based on one study by Zermansky 2006 (5). This study was conducted in residents of nursing care facilities with a mean age of 85. The intervention was a clinical medication review by a pharmacist consisting of a review of the GP advice and a consultation with the individual and residential carers. This recommendation was then forwarded to the residents GP. The control for this study was usual care. A second study identified in the Cochrane review was excluded from the analysis (Patterson 2010 (6)). This is because the intervention was specific to psychoactive medication. The value used in the analysis was the rate ratio 0.62 (0.53,0.72) demonstrating that a medication review by a pharmacist significantly reduced the rate of falling compared to usual care. The intervention used in the costing of the intervention included a RMMR by a pharmacist and a visit to the GP to correspond with the invention included in Zermansky 2006 (5). Multifactorial intervention The Cochrane review presents a number of meta-analyses for multifactorial interventions. Overall a nonsignificant rate of falls was observed compared to usual care. However, a subgroup analysis of multifactorial interventions have demonstrated a significant benefit (Dyer 2004, Jensen 2002 and McMurdo 2009) (7),(8),(9). These interventions include an exercise program, a medication review, modification of environmental hazards, personal care and protection (such as hip protectors), written materials for educational purposes, and an optical review. A recent meta-analysis (Vlaeyen 2015) also reported a reduction in falls from multifactorial intervention, with a reported RR of 0.67 (0.55, 0.82) (10) . This analysis included Dyer 2004(7) and McMurdo 2000(9), but also included two other studies (Becker 2003(11) and Neyens 2009(12)). The study by Becker 2003 was also added into the meta-analysis, however Neyens 2009 was excluded as it was not as comprehensive as the studies above and did not include a physical activity component. Figure 2 demonstrates the RR used in the Markov model. Figure 2. Comparison of Multifactorial interventions compared to usual care Hip-protectors The risk ratio used in the model for the effectiveness of hip protectors was sourced from a Cochrane review (13) and included 13 studies that compared hip protectors versus control (not wearing hip protectors) in institutional residences. Given that hip protectors reduce the number of fractures as opposed to the number of falls, the meta-analysis comparing hip protectors and the reduction in the rate of hip fractures was used. The risk ratio of 0.81 (0.66, 0.99) was applied directly in the model to reduce the number of hip fractures. This was achieved by adjusting the probability of being hospitalised after a fall in the model. The costing in the model reflected the cost of the hip protectors only, as it was assumed the fitting of the hip protectors by the nurses would be covered in the overall nurse wages. Probability of Falling The probability of falling each year was based on the statistic that 50% of residential aged care residents fall each year(14). This value was applied the medium risk group and the age group 75-79. The probability of falling in the low and high risk groups were extrapolated from the estimates of the medium risk group and adjusted to take into account that the absolute risk of being a faller if you fell in the past year was 71%, compared to 32% if you had not fallen in the past year. For the probabilistic sensitivity analysis a standard error of 0.10 was used to calculate the appropriate alpha and beta values for the beta distributions. Table 2 summarises the probability values used in the model for each age group. Table 2 Probability of Falling Age group 65-69 70-74 75-79 80-84 85+ Low risk 0.26 0.26 0.32 0.37 0.44 Medium risk 0.36 0.36 0.50 0.57 0.71 High risk 0.57 0.57 0.72 0.82 0.97 Utility values The starting utility at each cycle was based on an individual’s age at the beginning of that cycle minus a small decrement (0.072) for a fall in the previous year and a disutility (0.060) for being a resident in residential aged care. As individual’s moved through the decision tree a utility decrement was attributed to those who fell, received a minor injury and went the ED or were hospitalised. Population norms The population norms were sourced from Norman 2013 (15). These norms were estimated using the Household, Income and Labour Dynamics in Australia (HILDA) survey. Wave 9 was used in the analysis and was comprised of 17,630 individuals across 7,234 households. The respondents completed the SF36 and these values were converted into an SF-6D index score using the UK weighted algorithm . Hospitalisation decrement Average utility decrements were calculated using the population norms and reference health state values in Brazier 2002(16). These decrements were then weighted by the number of hip (94%) and vertebral fractures (6%) based on a population based study of hospitalised fall related injuries (17). This resulted in a hospitalisation decrement for these fractures of 0.144. Table 3 summarises these calculations. Table 3 Utility value for hospitalisation for fractures from a fall Age Population norms Population norms X Health state value hip fractures (0.797) 65-69 0.806 0.642 70-74 0.747 0.595 75-79 0.731 0.583 80-84 0.699 0.557 85+ 0.676 0.539 Average decrement Fracture decrement weighted by injury admissions (96% hip, 6% vertebral) Hip fracture decrement 0.164 0.152 0.148 0.142 0.137 0.149 Population norms X Health state value vertebral fracture (0.909) 0.733 0.679 0.664 0.635 0.614 Vertebral fracture decrement 0.073 0.068 0.067 0.064 0.062 0.067 0.144 Emergency attendance decrement The model assumed that the utility decrement for a wrist fracture would be used as the basis of an emergency attendance. Using the same methods as for the hospitalisation decrement and using a health state reference value of 0.977 from Strom 2007(18), the average wrist fracture decrement was 0.014. Previous fracture decrement Strom 2007(18) reported multipliers for subsequent years following a fracture. It was reported that a multiplier of 0.90 and 0.93 could be applied for hip and verterbral fractures respectively. Wrist fractures only received a disutility in the first year. The disutility for a previous fracture was calculated using the same methodology as the hospitalisation decrement above. The resulting decrement was calculated to be 0.072 and was applied in the model the year after a hospitalisation for a hip or vertebral fracture. References 1. Grieger JA, Nowson CA, Jarman HF, Malon R, Ackland LM. Multivitamin supplementation improves nutritional status and bone quality in aged care residents. Eur J Clin Nutr. 2009 Apr;63(4):55865. PubMed PMID: 18043700. 2. Bischoff HA, Stahelin HB, Dick W, Akos R, Knecht M, Salis C, et al. Effects of Vitamin D and Calcium Supplementation on Falls: A Randomized Controlled Trial. J Bone Miner Res. 2003;18(2):343-51. PubMed PMID: 12568412. 3. Broe KE, Chen TC, Weinberg J, Bischoff-Ferrari HA, Holick MF, Kiel DP. A higher dose of vitamin d reduces the risk of falls in nursing home residents: a randomized, multiple-dose study. J Am Geriatr Soc. 2007 Feb;55(2):234-9. PubMed PMID: 17302660. eng. 4. Flicker L, MacInnis RJ, Stein MS, Scherer SC, Mead KE, Nowson CA, et al. Should older people in residential care receive vitamin D to prevent falls? Results of a randomized trial. J Am Geriatr Soc. 2005 Nov;53(11):1881-8. PubMed PMID: 16274368. eng. 5. Zermansky AG, Alldred DP, Petty DR, Raynor DK, Freemantle N, Eastaugh J, et al. Clinical medication review by a pharmacist of elderly people living in care homes--randomised controlled trial. Age Ageing. 2006 Nov;35(6):586-91. PubMed PMID: 16905764. eng. 6. Patterson SM, Hughes CM, Crealey G, Cardwell C, Lapane KL. An evaluation of an adapted U.S. model of pharmaceutical care to improve psychoactive prescribing for nursing home residents in northern ireland (fleetwood northern ireland study). J Am Geriatr Soc. 2010 Jan;58(1):44-53. PubMed PMID: 20002510. 7. Dyer CAE, Taylor GJ, Reed M, Dyer CA, Robertson DR, Harrington R. Falls prevention in residential care homes: a randomised controlled trial. Age Ageing. 2004 November 1, 2004;33(6):596602. 8. Jensen J, Lundin-Olsson L, Nyberg L, Gustafson Y. Fall and injury prevention in older people living in residential care facilities. A cluster randomized trial. Ann Intern Med. 2002 May 21;136(10):733-41. PubMed PMID: 12020141. eng. 9. McMurdo ME, Millar AM, Daly F. A randomized controlled trial of fall prevention strategies in old peoples' homes. Gerontology. 2000 Mar-Apr;46(2):83-7. PubMed PMID: 10671804. eng. 10. Vlaeyen E, Coussement J, Leysens G, Van der Elst E, Delbaere K, Cambier D, et al. Characteristics and effectiveness of fall prevention programs in nursing homes: a systematic review and meta-analysis of randomized controlled trials. J Am Geriatr Soc. 2015 Feb;63(2):211-21. PubMed PMID: 25641225. 11. Becker C, Kron M, Lindemann U, Sturm E, Eichner B, Walter-Jung B, et al. Effectiveness of a multifaceted intervention on falls in nursing home residents. J Am Geriatr Soc. 2003 Mar;51(3):306-13. PubMed PMID: 12588573. eng. 12. Neyens JC, Dijcks BP, Twisk J, Schols JM, van Haastregt JC, van den Heuvel WJ, et al. A multifactorial intervention for the prevention of falls in psychogeriatric nursing home patients, a randomised controlled trial (RCT). Age Ageing. 2009 Mar;38(2):194-9. PubMed PMID: 19221130. 13. Gillespie WJ, Gillespie LD, Parker MJ. Hip protectors for preventing hip fractures in older people. Cochrane Database Syst Rev. 2010 (10):CD001255. PubMed PMID: 20927724. Epub 2010/10/12. eng. 14. Norton R, Butler M. Prevention of Falls and fall-related injuries among institutionalised older people. Wellington: University of Auckland; 1997. 15. Norman R, Church J, van den Berg B, Goodall S. Australian health-related quality of life population norms derived from the SF-6D. Aust N Z J Public Health. 2013 Feb;37(1):17-23. PubMed PMID: 23379801. 16. Brazier JE, Green C, Kanis JA. A Systematic Review of Health State Utility Values for Osteoporosis Related Conditions. Osteoporos Int. 2002;13:768-76. 17. Peel NM, Kassulke DJ, McClure RJ. Population based study of hospitalised fall related injuries in older people. Inj Prev. 2002;8:280-3. 18. Strom O, Borgstrom F, Sen SS, Boonen S, Haentjens P, Johnell O, et al. Cost-effectiveness of alendronate in the treatment of postmenopausal women in 9 European countries--an economic evaluation based on the fracture intervention trial. Osteoporos Int. 2007 Aug;18(8):1047-61. PubMed PMID: 17333449. eng.