SuperUser Support Guidelines for Nursing Documentation
advertisement

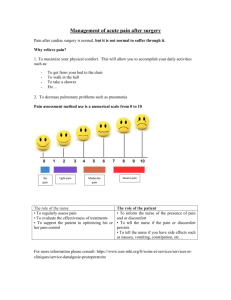
Nursing Documentation Revisions Super User Support Guidelines General Info Consult the SSS Support calendar and identify your SSS resource for the shift. Write down name and contact info. SSS will be rounding but one person will be covering multiple units. When you arrive notify the CSL that you are the Super User for that shift. You should NOT have a patient assignment but instead get a list of all the staff working on that shift. (Suggest printing from Vandy Works) If you are a super user on a unit whose routines are unfamiliar, ask CSL which shift is responsible for documenting the q24 discharge plan review. Denote which patients are scheduled for : o Transfers o Discharge o Procedures o Admissions Denote the nurse that has these patients since special documentation will need to be done and you may need to help coach the RN. We will support all users on the floor but the focus will be on the RNs. o Care Partners may notice the tab changes but they should use the Care Assistant Tab and it is NOT changing. o Med receptionist should not be impacted o Physicians and Ancillaries will have minimal impact unless they use HED to view data ( most don’t, most use starpanel flowsheets) If there is a technical problem and you know that the application is not working as it should, place a Help Desk Ticket. You may do this via calling or doing a self-serve ticket. If possible get exact steps the user did that resulted in problems. Try to reproduce the problem. Gather as much info as you can… Is this happening on all pt, one single pts, for all nurses, only one nurse etc. Denote the pt name, nurses name and the time of the issues. Call the SSS person if this is causing major issues with documenting care. Keep a note pad and document concerns, issues , questions you cant answeretc. Make sure to note any staff member with questions someone else will need to follow-up with so we can make sure they get the needed response. You will need to give a report to the oncoming super user as well as to the SSS person covering for your shift. When Rounding… Round with all RNs as they begin their shift – distribute job aides as needed Beginnings of shift verify: ALL RNS o Assess Care Categories in ALL CAPS + others based on problems or risk for problems o Denote Priority Problems for shift w/ !! & set goals for each priority problem. o Document Interventions in real time or near real time through the shift. o Check to assure that Normals are NOT being charted Review documentation for each nurse on at least on patient – try to do this with the nurse if possible. If not review and then give nurse feedback- start by asking how the nurse felt they did documenting with the changes. Did they experience issues or have questions, then give feedback. Be careful not to overwhelm if there were many opportunities for improvement. Focus on no more than 3 high impact issues. Re:Assessment – mid shift( per level of care standard) – ALL RNS o Timeframe for re-assessment • CU – at least two more times during the shift • Acute Care – at least once during the shift o Document either “unchanged” or “unchanged except” & denote changes for problems, risk for problems or based on orders &/or nursing judgment. DO NOT document on those WNL or WEL ( unless there is a change. o ICU – at least two more times during the shift o Acute Care – at least once during the shift Review documentation for each nurse on at least on patient. Assure that values from initial assessment are not repeated in the re-assessment. There should be only changes documented. Procedure or Transfer o Focused reassessment, note new, resolved, or unchanged problems o Summarize response to care focus on priority problems; Identify issues for f/u by receiving nurse; avoid duplication o Enter interventions, vitals, I&O, & meds Review documentation on case by case basis. • Remind nurse to inform receiving nurse how to look for data by viewing all tabs and selecting ALL DOCS . You may need to coach the receiving units too . • Sending Nurse documents transfer/transport in ALL DOCS tab or ADT tab • If patient went for a procedure and then returned assure that a focused reassessment is done. • If transferring from non implemented unit, remind RN to view sending unit documentation by clicking on “chart” in the tool bar and selecting the appropriate tab . Discharge o Summarize response to care, focus on unresolved problems and action plan post discharge; avoid duplication o Ensure all assessments, interventions, vitals, I&O, meds documentation is up-to-date o Transport section of All Docs completed Review documentation on case by case basis. New Admissions o Complete Admission History in StarPanel within 24 hrs. of admission o Assess ALL Care Categories, noting baseline status. If using WEL& OEL enter an annotation with supporting information as needed o Document Care Contact & VUMC general & unit specific orientation in Education Tab Review documentation on case by case basis. End of Shift o Summarize response to care focus on priority problems; Identify issues for f/u by receiving nurse; avoid duplication o Ensure all assessment, interventions, vitals, I&O, meds documentation is up-to-date Review documentation an hour or two before the end of the shift. Attempt to get with each nurse and give feedback – at minimal give feedback to those that you sense are struggling. Give Handover report to the super user that is coming on. Give handover report to the SSS person that is on your shift. ( see report form) NOTES: