Clinical Aspects of Acute pharyngitis
advertisement

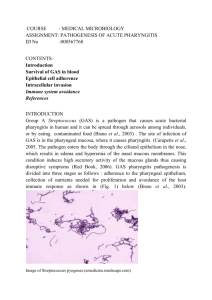
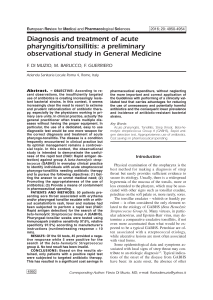
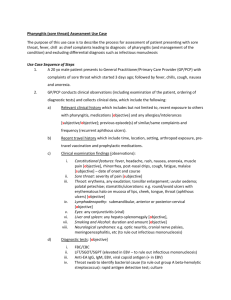
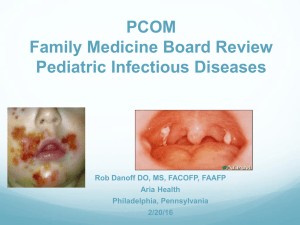
Clinical Aspects of Acute pharyngitis Group A [β]-hemolytic streptococci (e.g., S. pyogenes) are by a considerable margin the most frequent bacterial cause of acute pharyngitis, responsible for about 15-30% incidence rate in children and 5-17% in adults. Children are more susceptible to the condition due to their immature immune system having poor defence and low resistance towards the condition. They are first presented with an abrupt onset of fever and sore throat in either late winter or early spring. Clinical analysis of the condition in patients usually prioritises investigating for the clinical manifestation strep-throat, but the diagnosis of the disease is also based on other classic characteristics or signs; the presence of tonsillar exudates, tender anterior cervical lymph nodes, and absence of cough. These signs usually confirm the diagnosis as acute pharyngitis, with a strong association to group A streptococcal pharyngitis as the orchestrator of the disease. Other clinical manifestation includes nausea, pharyngeal hiperemis, abdominal pain, abdominal adenopathy, reddish and swollen tonsils, fever, rash of scarlet fever, sore throat, multiple enlarged tender cervical lymph nodes, swollen and red uvula, nasal obstruction, headache, raspy voice, malaise, pharyngeal erythema with/without petechiae on the palate, and pharyngeal chills. However, not all sufferers of acute pharyngitis display the full-blown syndrome or the classic signs of the condition as some have moderate form and are non-exudative (e.g., children below the age of three may have non-exudates, but may suffer from coryza with crusting of the nares, and adenopathy). Also exhibiting a lesser form of the disease are patients who had endure tonsillectomy. Nevertheless, these clinical presentations are due to the various virulence factors (e.g., Hyaluronic acid capsule defends the bacteria from phagocytises) that allow S. Pyogenes to attach to the host, and infiltrate the immune system causing the observed clinical symptoms. For example, the rash of scarlet fever and fever are caused by streptococcal pyrogenic exotoxin. In retrospect, the classic characteristics as well as the additional clinical factors such abdominal adenopathy may be valuable or beneficial in predicting the likelihood of the disease occurring (L. Bisno, 2001; Hafner, 2005; T. Shulman & R. Tanz, 1995). REFERENCES: Hafner, (2005) ‘The Clinical Diagnosis of Streptococcal Pharyngitis’, Annals of Emergency Medicine, pp. 87-89 L. Bisno, (2001) ‘Acute Pharyngitis’, Review Article, pp. 205 T. Shulman & R. Tanz, (1995) ‘Diagnosis and Treatment of Group A Streptococcal Pharyngitis’, Seminars in Pediatric Infectious Diseases, pp. 69