quality of life in elderly patients with chronic kidney disease: renal

O2
QUALITY OF LIFE IN ELDERLY PATIENTS WITH CHRONIC KIDNEY DISEASE:
RENAL REPLACEMENT THERAPY VS. CONSERVATIVE MANAGEMENT
Andrew Nixon
1
, Emma Dunn
2
.
1
Renal Medicine Department, Royal Preston Hospital, Preston,
United Kingdom.
2 Renal Medicine Department, St James’s University Hospital, Leeds, United
Kingdom.
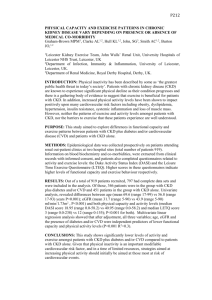
INTRODUCTION AND AIMS: Renal departments are encountering increasing numbers of elderly patients with chronic kidney disease (CKD). Recent evidence has demonstrated that any survival advantage that renal replacement therapy (RRT) has over conservative management may be lost in the elderly population with multiple co-morbidities. There are few studies that directly compare the symptoms and quality of life of elderly patients with advanced CKD managed conservatively with those managed with RRT. Given the limited evidence available, it can be challenging to help patients with CKD make informed treatment decisions. The aim of this study was to compare the symptoms and quality of life of patients with CKD aged ≥ 75 years old who were managed with RRT against those managed conservatively.
METHODS: A cross-sectional study was conducted. Three groups of patients ≥ 75 years old were included: patients with CKD managed conservatively (CM group), patients with CKD on haemodialysis (HD group) and patients with an eGFR ≤ 18 not yet requiring RRT (LC group).
All patients were asked to complete two validated quality of life scoring tools: POS-S Renal and
EORTC QLQ-C30. Chi-square tests of nominal independence were used to assess the patterns of responses within the patient groups. Fishers Exact Test was used to compare the pattern of responses of the LC group against the HD group and the CM group independently. A p-value of
<0.05 was considered statistically significant.
RESULTS: There were a total of 238 responses from a possible 351. All three groups reported the following symptoms frequently: tiredness, weakness and poor mobility. There were no statistically significant differences in the responses between the three groups for the majority of questions in both scoring tools (26 of 30 questions for EORTC QLQ-C30 and 16 of 17 questions for POS-S Renal). Notably, there were no significant differences between the three groups in the self-reported overall health score and the self-reported quality of life score. Both the HD group and CM group reported having more difficulty on concentrating on things
(p=0.03) and on remembering things (p=0.04) than the LC group. They also reported that their physical condition or medical treatment interfered more with their social activities (p=0.01) than the LC group. The only other statistically significant differences were found when directly comparing the HD group and the LC group. These differences were not found when comparing the CM group with the LC group. The HD group patients reported being more tired (p=0.02) and having more problems with weakness and lack of energy (p=0.03) than the LC group.
CONCLUSION: Patients with advanced CKD aged ≥75 years old who are managed conservatively do not have a higher symptom burden or a lower self-reported quality of life than those on haemodialysis. Nephrologists should clearly inform elderly patients with advanced
CKD that haemodialysis does not guarantee improved symptom burden or better quality of life.