Indication for Invasive Therapy

HCM
เรียบเรียงโดย นพ.อนันต์ ลาภพิกุลทอง
รศ.นพ.ธีรวิทย์ พันธุ์ชัยเพชร
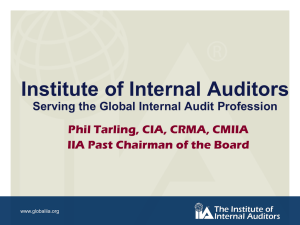
Definition of dynamic LVOT obstruction
Hemodynamic
State
Conditions Outflow
Gradient*
>30 mmHg Basal obstruction
Rest
Nonobstructive Rest
Physiologically provoked
Rest Labile obstructive
Physiologically provoked
* Peak-to-peak gradient
<30 mmHg
<30 mmHg
<30 mmHg
>30 mmHg
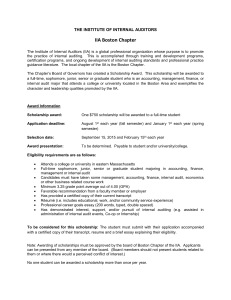
Indication for CAG or Coronary CTA
1.
Chest discomfort for intermediate risk of
CAD (I,C)
2.
CTA for chest discomfort and low risk of
CAD(IIa,C)
3.
Single photon emission computed tomography (SPECT) or positron
emission tomography (PET) myocardial perfusion imaging (MPI) for
chest discomfort and low risk of CAD
(IIa,C)
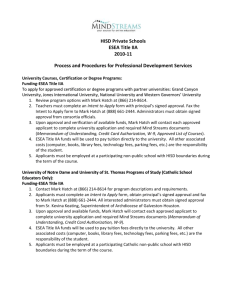
Indication for Invasive Therapy
Septal reduction therapy for severe drug- refractory symptoms and LVOT obstructions by
Experience operators(I,C)
* Experienced operators:
≥ 20 procedure or cumulative case
≥ 50 in HCM program
Eligible patients :
Clinical : Severe dyspnea or chest pain
(NYHA class III IV) or
occasionally other exertional symptoms
( syncope or near syncope)
Hemodynamic: Dynamic LVOT gradient at rest
>50 mmHg and SAM of the
mitral valve
Anatomic : anterior septal thickness sufficient to perform the procedure safely and effectively
Invasive therapy
1. 1 st choice Surgical septal myectomy,
(IIa,B)
2.
Symptomatic, severe resting obstruction
(>50 mm Hg) for whom standard medical therapy has failed(IIa,C)
3.
Alcohol septal ablation if septal myectomy is contra indicated (IIa,B)
4.
Alternative therapy : Alcohol septal ablation
(IIb,B)
Indication for Pacing
1.
Need pacing use dual chamber pacing to reduce LVOT obstruction (IIa,B)
2.
Alternative to invasive therapy : dual chamber pacing (IIb,B)
Selection patient for ICD
1.
documented cardiac arrest, VF, or hemodynamically
significant VT (I,B)
2. SCD in first degree relatives (IIa,C)
Maximum LV wall thickness >30 mm(IIa,C)
One or more recent, unexplained syncopal
episodes(IIa,C)
3. NSVT (age <30 y) in the presence of other
SCD risk factors (IIa,C)
4. Abnormal blood pressure response(>
20mmHg) with exercise in the
presence of other SCD risk factors
5.
Unexplained syncope, massive LV hypertrophy, or family history of SCD (IIa,C)
6.
NSVT with no SCD risk factors (IIb,C)
7.
significant outflow obstruction with abnormal blood pressure response during exercise in an absence of SCD risk factors (IIb,C)
SCD = Sudden cardiac death
NSVT = nonsustain VT - non sustain VT
CMR = Cardiac MR
SCD risk factors a.
LVOT obstruction
b.
Late gadolinium enhancement on CMR c.
LV apical aneurysm d.
Double and compound mutation
Recreational sports for HCM.
High = 0 - 1 (>6 METs) contraindication
Moderate = 4 to 5 (4-6 METs) accept
Low = 2 to 3 (<4 METs) individual consideration
Reference
1.
2011 ACCF/AHA Guideline for the
Diagnosis and Treatment of
Hypertrophic Cardiomyopathy