CL-12 Outline
advertisement

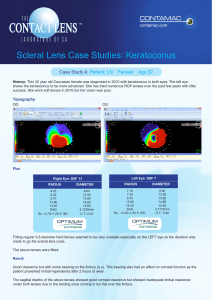
Understanding the basic and not so-basic essential tips in fitting scleral lenses. (1h00- modified) Abstract Despite a growth of 40% in the large diameter RGP lens category in the last year, a good number of practitioners are still shy to fit patients in this modality. In the past, lectures focused mainly on benefits of scleral lenses, their potential clinical applications, but not on basic to advanced fitting tips. This lecture aims to provide basic and advanced knowledge on scleral lens fitting, and to give some clinical pearls to help practitioners to start fitting these lenses with confidence. Issues that are most often seen are listed and ways to fix them are explored. A. Introduction 1. Understanding modern scleral designs a. New scleral lens education classification (corneo-scleral, miniscleral, scleral) b. Clinical applications for each types (i) Irregular corneas /ectasia (ii) Regular corneas (current refractive errors) (iii) Post surgery (iv) Specific populations: high ametropia, astigmatism presbyopia (v) Dry eye (vi) Diseased eyes 2. Pros and Cons vs other modalities a. Smaller GPs b. Hybrids c. Piggy backs B. Basic principles 1. Corneal and conjunctival 2. Sag vs Base curve anatomy C. Step-by-step approach for fitting large diameter contact lenses 1. Data from technology a. Evaluation of corneal and conjunctival profiles -topography b. Selection of initial B.C. /Sag/ diameter 2. Trial lens a. Empirical fitting is not an option b. Evaluation on the eye (i) OCT (ii)slit lamp D. Troubleshooting 1. Common to every types a. Handling b. Bubbles c. Tight lens syndrome d. Residual astigmatism e. Initial and long term discomfort f. Care regimen 2. Specific to smaller diameter lenses a. Limbal touch /compression 3. Specific to larger lenses a. Fogging b. Conjunctival toricity c. Blanching d. Oxygen permeability (vs compromised endothelium) E. Clinical applications (if time allows it) 1. Case Report #1 (Myopia, astigmatism and presbyopia) a.Caucasian, 54 YO, soft lens wearer (Proclear toric MF) b. Rx (i).OD -3.00 -2.00 x 10 (20/20); (ii) OS -2.50 -1.75 x 170 (20/20) (iii)Add +2.50 c.Main complaint: fluctuant vision (all distances), halos and glare at night d.Mini-scleral multifocal lens as a solution (i). No need to go larger (ii). Full compensation of refractive astigmatism (iii). Larger Optic Zone : reduces halos and glare (iv). Simultaneous aspheric design explained (v). Step by step fitting technique (vi). Lens used: One Fit Multifocal (Blanchard) 2. Case Report #4 (Keratoconus) a. Fitted in small RGP 20 years ago i) developed corneal scar OD b. Chronic discomfort and redness i) Tried piggy back and other type of lenses without success c. Recently grafted on one eye (OS) d. Mini scleral vs Large scleral lens options e. Lens used : One Fit KC (OD)- 14.6 mm and Acculens Maxim 7 (OS grafted) – 17 mm F. Conclusion 1. The selection of the right lens for the right patient eases the scleral lens fitting 2. Scleral lenses should be considered as a valid option to correct refractive error and to restore ocular and visual condition on a day-today basis 3. Mini-scleral and scleral lenses can be considered for the correction of regular refractive errors, not only for irregular corneas. 4. It is possible to define easy ways to fit and troubleshoot problems with large diameter contact lenses in order to prescribe them on a day-today basis. The first step being to consider the right lens for the right patient.