Controlled drinking: what commissioners need to
advertisement

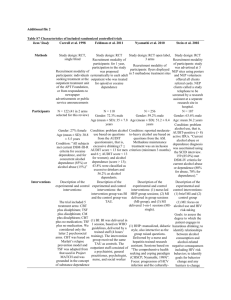
Reduction of alcohol consumption as a treatment approach for alcohol dependence: What commissioners need to know This document has been developed by Dr Carsten Grimm, Dr Steve Brinksman, Dr Lynn Owens and Dr Richard Watson (all members of the Integrated Care Pathway for the Prevention and Management of Alcohol Use Disorders in Adults Expert Advisory Group) with editorial support from Lundbeck Ltd. The Integrated Care Pathway tool was developed by the expert advisory group, which was convened and supported by Lundbeck Ltd. Lundbeck Ltd provided financial support for meeting costs, honoraria and administrative support of a medical communications agency. Lundbeck Ltd has reviewed the document for factual accuracy only. Executive summary Alcohol is a leading risk factor for death in people aged 15-49, and is a causal or component factor in >260 types of disease and injury. The absolute risk of dying from an alcohol-attributable disease or injury increases with increasing daily consumption, beyond just 10g (1¼ units) of alcohol. It has been estimated that alcohol misuse costs the NHS over £3.5 billion each year, and that there will be 210,000 potentially avoidable alcohol-related deaths between 2010 and 2030. While abstinence is the established treatment goal for alcohol-dependent patients, clinical studies and experience show that it is often difficult to achieve in the long-term. Problems include the difficulty that many dependent patients have in initiating abstinence-oriented treatment and in maintaining abstinence during and after treatment. A reduction-oriented approach to alcohol treatment is increasingly accepted as an effective management strategy for people with alcohol dependence. NICE discusses two treatment goals. It recommends abstinence as the appropriate goal for most people with alcohol dependence and significant co-morbidities. It also recommends moderate drinking for appropriate patients with mild alcohol dependence and no significant comorbidities. Reducing unhealthy alcohol consumption reduces health harms; it is associated with relatively quick (within weeks) improvements in blood pressure and depression, and also lowers the lifetime risk of developing serious and chronic diseases such as cancer (mouth, throat, oesophagus, liver and breast), cardiovascular disease, diabetes, epilepsy, stroke and liver disease. Reducing unhealthy alcohol consumption can bring significant public health and social benefits, including: fewer work, legal and financial problems, Document downloaded from: ‘Developing a Local Integrated Care Pathway for the Prevention and Management of Alcohol Use Disorders in Adults’ www.icp.alcoholconcern.org.uk fewer days’ absence from work due to alcohol-related illness, reduced levels of hospitalisation and less social harm. To date, most clinical studies evaluating interventions for alcohol dependence have been abstinence oriented and there has not been a research focus on potential reduction oriented approaches. Nevertheless, there is an ever-increasing evidence-base for reduction. o There is a significant evidence base for psychosocial therapies and NICE guidelines support the use of psychological and psychosocial therapies as the cornerstone of management of alcohol dependence. o Evidence for pharmacotherapies as adjunct to pychosocial therapies is also now increasing. 1. Introduction Reduced-risk drinking also referred to as controlled drinking or moderated drinking, refers “to the ability of an individual who has previously exhibited out-of-control drinking to return to a decreased, or more controlled pattern of alcohol consumption (1).” Although, historically, it has been a controversial subject, a reduction-oriented approach to alcohol treatment has been increasingly accepted as an effective management strategy for dependent drinkers, and it is now included in current NICE guidelines (see Box 1). The aim of this document is to summarise (a) the rationale and clinical evidence for a reduction of alcohol consumption as a relevant treatment goal and (b) the evidence for different interventions when studied in a reduction context (where this exists). Box 1: NICE CG115: 1.2.2.1 In the initial assessment in specialist alcohol services of all people who misuse alcohol, agree the goal of treatment with the service user. Abstinence is the appropriate goal for most people with alcohol dependence, and people who misuse alcohol and have significant psychiatric or physical comorbidity. When a service user prefers a goal of moderation but there are considerable risks, advise strongly that abstinence is most appropriate, but do not refuse treatment to service users who do not agree to a goal of abstinence. Document downloaded from: ‘Developing a Local Integrated Care Pathway for the Prevention and Management of Alcohol Use Disorders in Adults’ www.icp.alcoholconcern.org.uk 1.2.2.2 For harmful drinking or mild dependence, without significant comorbidity, and if there is adequate social support, consider a moderate level of drinking as the goal of treatment unless the service user prefers abstinence or there are other reasons for advising abstinence. 1.2.2.3 For people with severe alcohol dependence, or those who misuse alcohol and have significant psychiatric or physical comorbidity, but who are unwilling to consider a goal of abstinence or engage in structured treatment, consider a harm reduction programme of care. However, ultimately the service user should be encouraged to aim for a goal of abstinence. 2. Rationale and clinical evidence for reduction of alcohol consumption as a relevant treatment goal 2.1 Prolonged heavy drinking is associated with poor long-term health and carries a significant economic and social burden Alcohol is the world’s leading risk factor for death in people aged 15-49 (2). In the EU, alcohol consumption is cited as the third highest risk factor for ill-health after high bloodpressure and tobacco use (3). According to the World Health Organization, alcohol is a causal factor in >60 types of disease and injury and is a component cause in 200 others (4). The amount of alcohol consumed is one of the key risk factors for poor health outcomes (drinking pattern is also important). Indeed, a dose-dependent relationship between level of alcohol consumption and disease risk has been shown for most categories of disease (including liver disease, cardiovascular disease, cancer, and suicide), with higher alcohol consumption conferring more risk (5). The absolute risk of dying from an alcoholattributable disease or injury has been shown to increase with increasing daily consumption (above 10g of pure alcohol) (6). It is clear that alcohol dependence causes significant burden to healthcare expenditure and society. In England, it has been estimated that up to 5.9% of the population have alcohol dependence (7, 8). It is further estimated that alcohol misuse costs the NHS over £3.5 billion each year (9), and that there will be 210,000 potentially avoidable alcohol-related deaths between 2010 and 2030 (10). Document downloaded from: ‘Developing a Local Integrated Care Pathway for the Prevention and Management of Alcohol Use Disorders in Adults’ www.icp.alcoholconcern.org.uk 2.2 Abstinence can be difficult for many dependent drinkers to achieve; controlled-drinking offers a practical and effective management strategy Abstinence is the established treatment goal for alcohol-dependent patients (8). However, it is often difficult to achieve in the long-term. Studies show that when a goal of abstinence is imposed on the patient, fewer than half will remain abstinent after 5 years (11). Such problems with this “all or nothing” approach mean that it is now increasingly accepted that treatment success in alcohol dependence should be considered as a continuum, where a reduction in alcohol consumption is deemed a positive interim outcome (5). A key barrier to achieving a successful outcome with abstinence-based therapy is that it is often difficult for alcohol-dependent patients to initiate abstinence; many are either not interested in abstinence at the time of entering treatment or unable to commit to abstinence at the time of entering treatment. In one UK study, 45.7% of patients enrolled stated that they preferred a non-abstinence goal (12). Patients are more likely to remain engaged in treatment when they are presented with more than one treatment option and are given a degree of responsibility and control over treatment decisions, so by giving them an option there is the potential to encourage more dependent drinkers to seek professional help and enter treatment programmes. (1). Evidence also suggests that patients are more likely to achieve self-set goals, rather than goals that are imposed on them (13, 14). Reduction oriented treatment has been shown to act as an effective ‘bridge’ on route to abstinence. Studies show that when patients are allowed to gradually reduce their alcohol consumption more patients will achieve a positive outcome (abstinence and controlleddrinking) than those who stop drinking suddenly, but the proportion achieving abstinence is similar (15). In a randomized, controlled trial that compared the effectiveness of abstinence with reduction as treatment goals, no significant differences were found between the two groups in reported alcohol consumption at the end of the study (16). Crucially, although the drinking outcomes of the groups were similar, reduction of alcohol consumption was considered by the patients to be a more suitable and acceptable goal (most of the clients assigned to abstinence rejected this goal from the outset) (16). It is also important to recognize that the patient’s own treatment goals are not necessarily static. In one Canadian study patients who initially chose reduction as their treatment goal later changed their goal to abstinence, indicating that positive experiences during treatment Document downloaded from: ‘Developing a Local Integrated Care Pathway for the Prevention and Management of Alcohol Use Disorders in Adults’ www.icp.alcoholconcern.org.uk can impact on an individual’s goals (13). The authors of the study concluded, “that there is value in helping individuals move toward an appropriate goal (given their level of severity of problem) rather than imposing a goal at the beginning of treatment” (13). 2.3 Reducing unhealthy alcohol consumption reduces the risk for a variety of serious health problems in both the short- and longer-term Accumulating evidence shows that reducing unhealthy alcohol consumption not only brings relatively quick (within weeks) improvements in blood pressure (17) and depression (18), but also lowers the lifetime risk for developing serious and chronic diseases, including cancer, cardiovascular disease, diabetes, epilepsy, stroke and liver disease (5, 6). This is supported by a Cochrane analysis of brief interventions for heavy alcohol users which found that patients in the treatment group had a greater reduction in their alcohol intake with significantly fewer deaths at 6 months and 1 year versus the control group (19). Likewise, in an analysis that combined data from seven large, multisite, abstinence-based studies (8389 patients), 75% of study participants had ongoing episodes of drinking but managed to reduce their overall alcohol consumption by 87%, with a corresponding 60% decrease in alcohol-related problems (20). Long-term follow up studies also demonstrate the medico-social benefits of controlleddrinking. A 5-year naturalistic study of 850 Spanish patients enrolled in an abstinenceoriented treatment program found that patients who did not attain abstinence but achieved controlled-drinking had significantly fewer emergency room visits, hospitalizations and work problems (including absenteeism and sick leave) compared to those who continued to drink heavily (11). Similar benefits have also been reported in a 5-year study of Swedish middleaged male heavy drinkers who were enrolled in a program designed to encourage a reduction in their drinking. In this study, patients were identified by screening for elevated GGT levels and were randomized to the treatment program (with a goal of moderate drinking) or no further intervention (control). Compared with the control group, patients who received the intervention had 60% fewer hospital days at 5 years, including fewer hospital days for mental disorders, accidents or injuries and alcohol-related diseases. Overall, patients in the control group had about 4 times as many hospital days as the men in the intervention group. Furthermore, the mortality was twice as great in the control group during the follow-up period (21). Document downloaded from: ‘Developing a Local Integrated Care Pathway for the Prevention and Management of Alcohol Use Disorders in Adults’ www.icp.alcoholconcern.org.uk 3. Evidence for existing interventions when studied in a reduction context 3.1 Current approaches to the management of alcohol dependency In their appraisal, NICE reviewed the evidence for psychological and psychosocial interventions as well as pharmacological therapy for the management of harmful drinking and alcohol dependence (8). To date, most studies have been abstinence oriented and there has not been a research focus on potential reduction oriented approaches (1). Nevertheless, there is an ever-increasing evidence-base for reduction, which is briefly outlined below. When evaluating the evidence, it is important to note a number of methodological issues, which make it hard to directly compare studies. Firstly, there is significant heterogeneity in the patient populations studied; for example different studies included opportunistic or help-seeking populations, patients with varying levels of risk (hazardous, harmful, mild dependence, severe dependence) and patients with different co-morbidities. Secondly, the outcome measures used vary depending on the stated goal of therapy. Studies focused on abstinence will frequently use Relapse or Return to heavy drinking as primary outcome measure. However, the outcomes more relevant to reduction include: heavy drinking days (HDD), total alcohol consumption (TAC), drinking days, liver enzymes and Clinical Global Impression (CGI) (5). Finally, there is also significant variation in duration of studies and length of follow-up and the intensity (frequency) of treatment. 3.2 Psychological and psychosocial approaches NICE guidelines support the use of psychological and psychosocial therapies as the cornerstone of management of alcohol dependence (8). Using meta-analytic approaches, they concluded that there was “evidence that cognitive behavioural therapy (CBT), social behaviour and network therapy (SBNT), and behavioural therapies were better than treatment as usual or control.” (8). Looking at the rates of alcohol consumption posttreatment (i.e. outcome measures more relevant to controlled drinking), NICE found that CBT were significantly better than control at reducing heavy drinking episodes but no significant difference between groups was observed for a reduction in days any alcohol is used (assessed post-treatment) or the number of participants who have lapsed and relapsed (assessed at 3-month follow-up) when compared with treatment as usual (8). Likewise, behavioural therapies were found to be more effective than control in reducing the amount Document downloaded from: ‘Developing a Local Integrated Care Pathway for the Prevention and Management of Alcohol Use Disorders in Adults’ www.icp.alcoholconcern.org.uk of alcohol consumed (SMD = 0.97, large effect size) and maintaining reduced drinking (SMD = 0.60, medium effect size) when assessed post-treatment (8). With regards to other forms of psychological and psychosocial therapies, NICE concluded, ”there was very limited evidence of low-to moderate quality to support the efficacy of counselling, short-term psychodynamic therapy, multi-modal treatment, self-help based treatment, psychoeducational interventions and mindfulness meditation” (8). For a full overview of the evidence for psychological and psychosocial approaches readers are referred to the full NICE guidance [insert hyperlink here]. 3.3 Pharmacological approaches Whereas a reduction of alcohol consumption is a more frequent goal in psychosocial approaches, the vast majority of pharmacotherapy trials (naltrexone, acamprosate and disufiram) have been evaluated in an abstinence-oriented manner. At present NICE guidelines recommend offering either acamprosate or oral naltrexone in combination with an individual psychological intervention focused specifically on alcohol misuse to people with moderate and severe alcohol dependence after a successful withdrawal (8). 3.3.1 Systematic reviews Systematic reviews for naltrexone, acamprosate and disulfiram have been performed. [Click here to access the Cochrane reviews of naltrexone and acamprosate]. Links to be added In brief, the Cochrane review of naltrexone therapy was based on 50 randomized controlled trials (7793 patients) and found that treatment with naltrexone reduced the risk of heavy drinking to 83% of the risk in the placebo group and decreased drinking days by about 4% (22). However, the review also found that gastrointestinal symptoms like nausea, stomach pain and loss of appetite are common and that some patients feel tired when taking naltrexone (22). Likewise, the Cochrane review of acamprosate concluded that although treatment with acamprosate was shown to significantly reduce the risk of any drinking and increase the cumulative abstinence duration versus placebo, there was no statistical difference in heavy drinking (23). In an independent systematic review of 11 randomized controlled trials of disulfiram for alcohol dependence, only 6 studies reported a significant better effect of treatment with disulfiram on abstinence than placebo (24). One study found that treatment with disulfiram 250mg resulted in significantly fewer drinking days Document downloaded from: ‘Developing a Local Integrated Care Pathway for the Prevention and Management of Alcohol Use Disorders in Adults’ www.icp.alcoholconcern.org.uk (secondary outcome measure) in patients who had completed all 7 follow-up interviews during the 12 months (24). 3.3.2 Randomized controlled trials Few trials have compared the efficacy of available treatments. A randomized multicentre open-label, comparative trial of naltrexone, acamprosate and disulfiram in the treatment of alcohol dependence was conducted to directly compare their efficacy when used with a brief manual-based cognitive-behavioural intervention (25). The study was conducted in two main phases; a 12-week continuously supervised medication, followed by targeted medication up to 52 weeks and a 67-week follow-up period (i.e. total of 2.5 years). All three groups showed marked reduction in drinking, from baseline to the end of the study. During the continuous medication phase, treatment with disulfiram was more effective in reducing HDDs and average weekly alcohol consumption, and increasing time to the first drink, as well as the number of abstinent days. During the targeted medication phase, there were no significant differences between the groups in time to first HDD and days to first drinking, but the abstinence days were significantly more frequent in the disulfiram group. There were no differences between the naltrexone and acamprosate groups in either phase of the study of drinking outcomes (25). The COMBINE Study (26) was a randomized controlled trial conducted to evaluate the efficacy of naltrexone, acamprosate, behavioural therapies, and their combinations for treatment of alcohol dependence. Eight groups of patients received medical management with 16 weeks of naltrexone (100 mg/d) or acamprosate (3 g/d), both, and/or both placebos, with or without a combined behavioural intervention (CBI). A ninth group received CBI only (no medication). All groups showed substantial reduction in drinking. During treatment, patients receiving naltrexone plus medical management, CBI plus medical management and placebos, or both naltrexone and CBI plus medical management had more days abstinent than those receiving placebos and medical management only. Naltrexone also reduced risk of a HDD over time, this was most evident in those receiving medical management but not CBI. Conversely, acamprosate showed no significant effect on drinking versus placebo, either by itself or with any combination of naltrexone, CBI, or both (26). Document downloaded from: ‘Developing a Local Integrated Care Pathway for the Prevention and Management of Alcohol Use Disorders in Adults’ www.icp.alcoholconcern.org.uk References 1. Ambrogne JA. Reduced-risk drinking as a treatment goal: what clinicians need to know. J Subst Abuse Treat. 2002; 22(1):45-53. 2. Lim SS, Vos T, Flaxman AD, Danaei G, Shibuya K, Adair-Rohani H, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2013; 380(9859):2224-60. 3. WHO. Alcohol in the European Union: Consumption, harm and policy approaches 2012. 2012. 4. WHO. Global Status Report on Alcohol & Health, 2011 5. Gastfriend DR, Garbutt JC, Pettinati HM, Forman RF. Reduction in heavy drinking as a treatment outcome in alcohol dependence. J Subst Abuse Treat. 2007; 33(1):71-80. 6. Rehm J, Baliunas D, Borges GL, Graham K, Irving H, Kehoe T, et al. The relation between different dimensions of alcohol consumption and burden of disease: an overview. Addiction. 2010; 105(5):817-43. 7. Fuller E, Jotangia D, Farrell M. Alcohol misuse and dependence. In: McManus S, Meltzer H, Brugha T, Bebbington P, Jenkins R, editors. Adult psychiatric morbidity in England, 2007: Results of a household survey. London: The NHS Information Centre for health and social care; 2009. 8. NICE. Clinical Guideline 115. Alcohol-use disorders. Diagnosis, assessment and treatment of harmful drinking and alcohol dependence. February 2011. http://www.nice.org.uk/nicemedia/live/13337/53191/53191.pdf 2011. 9. NHS. The Health & Social Care Information Centre. Statistics on Alcohol: England, 2011. 10. Sheron N, Gilmore I, Parsons C, Hawkey C, Rhodes J. Projections of alcoholrelated deaths in England and Wales--tragic toll or potential prize? Lancet. 2012; 379(9817):687-8. 11. Gual A, Lligona A, Colom J. Five-year outcome in alcohol dependence. A naturalistic study of 850 patients in Catalonia. Alcohol Alcohol. 1999; 34(2):183-92. 12. Heather N, Adamson SJ, Raistrick D, Slegg GP. Initial preference for drinking goal in the treatment of alcohol problems: I. Baseline differences between abstinence and non-abstinence groups. Alcohol Alcohol. 2010; 45(2):128-35. 13. Hodgins DC, Leigh G, Milne R, Gerrish R. Drinking goal selection in behavioral self-management treatment of chronic alcoholics. Addict Behav. 1997; 22(2):247-55. 14. Al-Otaiba Z, Worden BL, McCrady BS, Epstein EE. Accounting for self-selected drinking goals in the assessment of treatment outcome. Psychol Addict Behav. 2008; 22(3):439-43. 15. Sobell MB, Sobell LC. Second year treatment outcome of alcoholics treated by individualized behavior therapy: results. Behav Res Ther. 1976; 14(3):195-215. 16. Sanchez-Craig M, Annis HM, Bornet AR, MacDonald KR. Random assignment to abstinence and controlled drinking: evaluation of a cognitive-behavioral program for problem drinkers. J Consult Clin Psychol. 1984; 52(3):390-403. 17. Xin X, He J, Frontini MG, Ogden LG, Motsamai OI, Whelton PK. Effects of alcohol reduction on blood pressure: a meta-analysis of randomized controlled trials. Hypertension. 2001; 38(5):1112-7. Document downloaded from: ‘Developing a Local Integrated Care Pathway for the Prevention and Management of Alcohol Use Disorders in Adults’ www.icp.alcoholconcern.org.uk 18. Brown SA, Schuckit MA. Changes in depression among abstinent alcoholics. J Stud Alcohol. 1988; 49(5):412-7. 19. McQueen J, Howe TE, Allan L, Mains D, Hardy V. Brief interventions for heavy alcohol users admitted to general hospital wards. Cochrane Database Syst Rev. 2011; (8):CD005191. 20. Miller WR, Walters ST, Bennett ME. How effective is alcoholism treatment in the United States? J Stud Alcohol. 2001; 62(2):211-20. 21. Kristenson H, Ohlin H, Hulten-Nosslin MB, Trell E, Hood B. Identification and intervention of heavy drinking in middle-aged men: results and follow-up of 24-60 months of long-term study with randomized controls. Alcohol Clin Exp Res. 1983; 7(2):203-9. 22. Rosner S, Hackl-Herrwerth A, Leucht S, Vecchi S, Srisurapanont M, Soyka M. Opioid antagonists for alcohol dependence. Cochrane Database Syst Rev. 2010; (12):CD001867. 23. Rosner S, Hackl-Herrwerth A, Leucht S, Lehert P, Vecchi S, Soyka M. Acamprosate for alcohol dependence. Cochrane Database Syst Rev. 2010; (9):CD004332. 24. Jorgensen CH, Pedersen B, Tonnesen H. The efficacy of disulfiram for the treatment of alcohol use disorder. Alcohol Clin Exp Res. 2011; 35(10):1749-58. 25. Laaksonen E, Koski-Jannes A, Salaspuro M, Ahtinen H, Alho H. A randomized, multicentre, open-label, comparative trial of disulfiram, naltrexone and acamprosate in the treatment of alcohol dependence. Alcohol Alcohol. 2008; 43(1):53-61. 26. Anton RF, O'Malley SS, Ciraulo DA, Cisler RA, Couper D, Donovan DM, et al. Combined pharmacotherapies and behavioral interventions for alcohol dependence: the COMBINE study: a randomized controlled trial. JAMA. 2006; 295(17):2003-17. Document downloaded from: ‘Developing a Local Integrated Care Pathway for the Prevention and Management of Alcohol Use Disorders in Adults’ www.icp.alcoholconcern.org.uk