perioperative paper
advertisement

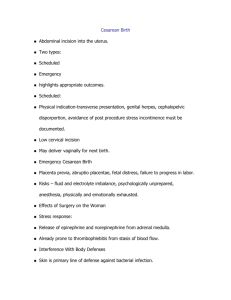
1 Running Head: OPERATING ROOM REPORT Perioperative Care with a Hysterectomy and Cystoscopy Kiersten Carbone Saint Joseph’s College of Maine Nursing of the Adult I Clinical Victoria Ramsay October 26, 2010 2 Running Head: OPERATING ROOM REPORT Perioperative care with a Hysterectomy and Cystoscopy Perioperative Considerations This paper focuses on a fifty-one year old female with a scheduled hysterectomy and cystoscopy. The goal of this surgery is remove her uterus and to examine her bladder. For any operative procedure it is important to obtain the patients past medical history. In this case, the patient’s history includes GERD, HTN, hyperlipidemia, three cesarean sections (9/86, 10/87, and 11/88), a Bilateral Tubular Ligation, and herniorrhaphy. Her home medications include Lipitor 10 mg by mouth daily for hyperlipidemia, Atenolol 25 mg by mouth daily for HTN, Aspirin 81 mg for bleeding and prevention of MI/SVA, Micardic HCT 40/12.5 M by mouth daily for HTN, Ferrous Sulfate 325 mg by mouth daily for iron deficiency anemia, Provera for dysfunctional uterine bleeding, and Venofer IV weekly for one month for iron deficiency anemia. This patient was having surgery to remove her uterus due to bleeding (menorrhagia) which resulted in iron deficiency anemia related to symptomatic fibroids. The plan of this procedure is to remove her uterus by way of a laprascopic, supracervical hysterectomy through three incisions in her abdomen. A major impact on the patient after this surgery is that she will no longer be able to get pregnant. Although due to her previous bilateral tubular ligation surgery, this will not be a problem for her because she can already no longer become pregnant. One consideration that can be taken is how it is going to impact the patient’s view of her femininity and how this could alter her body image (Lewis et al, 2007). Along with this, one must consider how it is going to affect the intimate relationship between the patient and her husband. She may feel depressed and have a loss in sexual pleasure. Along with this surgery, there are variables to consider that could increase the patient’s risks for operative complications. Although most women do not have health problems during or after the surgery, there are a few to consider. One variable is the risk for a deep vein thrombosis. According to Lewis, Heitkemper, Dirksen, O’Brien, & Bucher (2007), these “may form in the leg veins as a result of inactivity, body position, and pressure, all of which lead to venous stasis and decreased tissue perfusion”(p. 384). This patient is at an even higher risk due to being immobile during the surgery and her obesity, potentially resulting in a pulmonary embolism. Another factor to keep in mind is injury to nearby 3 Running Head: OPERATING ROOM REPORT organs such as the bowel, urinary tract, bladder, rectum, blood vessels, ovaries, and cervix (Trimble, 2009). With this surgery, you come in contact with a number of other organs, increasing the risk for damage to them and bleeding internally. This is why it is important for the surgeon to make cuts carefully and precisely. A final and major risk factor is the risk for infection. “Our skin is considered our protective barrier; therefore wound healing is a major concern when an incision is made” (Lewis et al., 2007, p. 392). According to Lewis et al. (2007), along with this incision, infection may result from a number of sources, such as: “exogenous flora present in the environment and on the skin, oral flora, and intestinal flora” (p. 392). This patient is at an even higher risk, due to her history of three cesarean sections. Due to her scarring, there is a chance that the scar tissue could break open, resulting in an even slower wound healing process and increase risk for infection. Along with all surgical procedures, adequate teaching is critical. Specific preoperative teaching that should be done before a hysterectomy is performed is to educate the patient on the reason for having a hysterectomy, what the procedure consists of, and how the operation will be executed. In this patient’s case, she is having her uterus removed due to excessive bleeding and iron deficiency anemia related to symptomatic fibroids. This will be executed by operating laparoscopically with three incisions. It is also important to make sure they are aware that once there uterus is removed they will no longer be able to become pregnant. In this patient’s case, this does not affect her due to having her tubes tied in a previous surgery. The patient should also be aware of the type of anesthesia that will be used and how it will affect her body. Another aspect of teaching is to make sure the patient is aware of how she will be monitored postoperatively. Vital signs will be assessed to make sure she is stable, wound checks for bleeding or infection, their urinary output is adequate, and the patient is alert and responsive. Also general postoperative nursing care should be reviewed including how the patient should be positioned, coughing, deep breathing, how to use an incentive spirometer to prevent atelectasis, dressing care, and the importance of mobility. It is also important to teach the patient about what to expect after the surgery, such as acute pain related to the incision site, nausea related to effects of anesthetic agents, insertion of a 4 Running Head: OPERATING ROOM REPORT Foley catheter, and decreased ambulation due to pain. The nurse is responsible for making sure the patient is educated on each one of these aspects and shows a good understanding before undergoing the surgery. In addition to pre-op teaching, there are essential items to check immediately before the patient is transferred into the operating room. According to Lewis et al. (2007), five items that the nurse should check before the patient leaves for the operating room include: 1) the patient has a signed consent form in the charts. Without this form, providers are not allowed to proceed; 2) all of the patient’s personal belongings are removed and their location are documented on a sheet of paper; 3) the patient is wearing an identifying name band; 4) the surgery site on the patient is marked; and 5) all diagnostic laboratory results are available along with the preoperative medications that were administered. Lewis et al. (2007) includes a comprehensive example of a preoperative checklist that includes these relevant aspects of preoperative care (p. 355). In addition, this patient had a completed preoperative checklist on the front of her chart. It was completed and signed by a registered nurse and facilitated safe care because all of the required items were checked and easily communicated to the surgical team. One vital element of the preoperative checklist is the informed consent. This patient did have a signed informed consent in her chart. It was obtained by a physician and included three conditions 1) adequate disclosure of the diagnosis, information about the treatment and its risks, and why the surgery is being done, 2) clear and comprehensible information about the procedure, and 3) voluntary consent by the patient (Lewis et al., 2007, p. 353). In order to be legal, this form must be signed by the patient undergoing the surgery. Her consent was appropriately signed and in the medical record. Before proceeding into the operating room, it is important to make sure the patient has a list of medications to be given preoperatively. This patient received a number of medications before her surgery. First, she was given her Atenolol since she had not taken any of her medications since Sunday because she thought they would give her an upset stomach. This medication is to keep her hypertension under control. Specifically for the procedure, she was administered GoLYTELY the night before as a bowel preparation for her GI surgery. Major side effects to monitor for are abdominal fullness, diarrhea, nausea and vomiting (Deglin, 2009). The morning before the surgery she received three medications. First she 5 Running Head: OPERATING ROOM REPORT received Cefoxitin (Mefoxin) 2 g as a perioperative prophylaxis to prevent intra-abdominal and gynecologic infections (Deglin, 2009). Major side effects to be aware of include seizures, pseudomembranous colitis, diarrhea, rashes, and bleeding (Deglin, 2009). Then she received Versed (midazolam) for preoperative sedation, anxiolysis, and amnesia (Deglin, 2009). Major adverse reactions that need to be monitored after receiving versed include drowsiness, excess sedation, headache, blurred vision, apnea, laryngospasm, respiratory depression, and hypotension (Deglin, 2009). This medication really helps to relax the patient and helps them to not remember anything about the procedure. Lastly she received Fetanyl, which is a supplement in anesthesia and helps to decrease pain (Deglin, 2009). Adverse side effects to be aware of and monitor for include confusion, postoperative depression, blurred/doubled vision, apnea, laryngospasm, respiratory depression, arrhythmias, biliary spasm, and facial itching (Deglin, 2009). Each one of these medications carried out specific roles to help the surgery go more smoothly. Intraoperative Considerations The personnel in the OR during the patient’s surgery included two GYN surgeons, who actually performed the removal of the uterus. One took control of the actual removal of the uterus and held the camera while the other assisted by rotating the uterus. These two surgeons were also assisted by one certified scrub technician who helped by handing the surgeon the tools that she needed and suctioning the extra fluid and smoke within the surgical site. The anesthesiologist was in charge of keeping the patient’s vital signs stable and administering the intraoperative medications to keep the patient sedated and comfortable during general anesthesia. He was located at the head of the bed surrounded by a number of monitoring systems including a cardiac monitor. There was one circulating nurse in the room who made sure that the other members of the team had everything they needed and documented information on the computer. Also there was a floating OR nurse who would come in and work with the circulating nurse or give her a break and take over what she had been doing. In the operating room, safety measures and infection control are extremely important to ensure a safe and sterile procedure for the patient and team. The first precaution was a white board in the room 6 Running Head: OPERATING ROOM REPORT where the certified scrub technician counted all of the tools that were being used and reported the number to the circulating nurse who would write down the number of each tool on the board and at the end of the procedure they made sure to account for all of the tools. Then all team members who would possibly be coming into contact with the patient, scrubbed up and once they did, they did not leave the room or touch anything that wasn’t sterile. Everything sterile in the room was on a blue or green sterile field, everyone who was not sterile in the room kept far away from these zones. When setting up the sterile tables and equipment for the procedure, the nurse made sure there was a safe circulating path around the patient and all wires were taped down. Also when walking around the room, the nurse and I walked as close to the wall as we could with our front side facing the field, to make sure we did not come in contact with anything sterile. Before the team began the procedure, everyone stopped what they were doing and called a surgical time. According to Lewis et al. (2007), this is done to “verify patient identification, surgical procedure, and surgical site. This is now considered a Universal Protocol and is done prior to all invasive procedures to ensure safety and accuracy as stated by Lewis et al. (2007). At that time all team members went through the pertinent patient information to make sure that this was the right patient, the right procedure, and the right site before making the incisions and moving forward with the procedure. Another important safety measure is the positioning of the patient before the procedure begins. As Lewis et al. (2007) states, “care must be used to provide skeletal alignment, prevent pressure on nerves, skin over bony prominences and eyes, provide for adequate thoracic excursion, prevent occlusion of arteries/veins, provide modesty in exposure, and recognize and respect individual needs such as previously assessed aches, pains, or deformities” (p. 366). It is the nurses’ responsibility to make sure this is carried out. When positioning this patient, she was first placed in the supine position when transferred onto the OR bed. While in this position they had her remove her underwear and applied pneumonic compression devices to each calf to prevent any DVTS or pulmonary embolisms throughout the procedure. After she received the anesthesia she was moved into the lithotomy position so that they were able to give her a pelvic exam and perform the procedure laparoscopically through her abdomen. First they moved her down the bed so that her buttock was placed just above the foot of the bed. Then they 7 Running Head: OPERATING ROOM REPORT detached the foot of the bed and attached the foot stirrups where her feet and legs were placed. Lastly, they tucked her arms in next to her sides on the removable cushions that were attached to keep them out of the way and out of harm. Observing this hysterectomy procedure was so exciting and very interesting to see how it was performed. First the surgeon made an incision in the base of the belly button. Then two more incisions were made near the hip bones. Then once ports are placed in these incisions sites they go in with different tools and a camera to separate the uterus from its blood supply and the cervix. This is very carefully done with a tool that the surgeon uses to either cut or coag (burn) it to separate the uterus from the abdomen and cervix. When doing so, the other surgeon is assisting her and rotating the uterus to make sure it is fully detached. Once the uterus is detached the surgeon comes in with another tool called the GYRUSACMI. While one surgeon holds the uterus, the other uses this tool to grab pieces of it and cuts it up into strips which are then pulled out through the port in the incision and placed in a bowl that the certified scrub technician holds. Once this is completed and all pieces are removed, the hysterectomy part is done. Then they performed a cystoscopy to examine the bladder and make sure there are no abnormalities. Lastly, they insert a dye to make sure that the urinary tract system is working properly. To do so they place the camera in the bladder and sit and wait for each ureter to secrete urine into the bladder. Once they were assured both ureters were working, they removed all tools, and sewed the patient back up and the procedure was completed. This patient received general anesthesia and local anesthesia. According to Lewis et al. (2007), general anesthesia “is the loss of sensation with loss of consciousness; skeletal muscle relaxation; possible impaired ventilatory and cardiovascular function; and elimination of the somatic, autonomic, and endocrine responses” (p. 367). The actual drugs were not revealed to me, but I do know a number of different ones were used. General side effects to monitor while a patient is under anesthesia are for adverse cardiac effects, tachycardia, bradycardia, hypotension, nausea and vomiting, respiratory depression, and hiccups (Lewis et al, 2007). The other anesthesia that this patient received was bupivacaine, which was given to her through an epidural catheter. This drug is classified as a therapeutic 8 Running Head: OPERATING ROOM REPORT epidural local anesthetic. It “inhibits initiation and conduction of sensory nerve impulses by altering the influx of sodium efflux of potassium in the neurons” (Deglin, 2009, p 1021). Side effects to monitor with this drug include seizures, dizziness, headache, blurred vision, cardiovascular collapse, arrhythmias, bradycardia, hypotension, tachycardia, urinary retention, pruritus, and metabolic acidosis (Deglin, 2009). The nursing considerations for this anesthetic include “assessing the patient for toxicity, monitoring the patient for orthostatic hypotension, and monitoring blood pressure, heart rate, and respiratory rate” (Deglin, 2009, p. 479). Important aspects to watch for postoperatively with any general anesthesia are to make sure that the patient has a patent airway and that the patient can adequately breathe. With an epidural catheter, it is critical to monitor respiratory excursion, because if there is too high of a block it can result in inadequate breathing or apnea (Lewis et al, 2007). Therefore oxygen saturation and respiratory rate should be monitored closely. After the procedure was over the patient began to start waking up. The patient was then transferred to the post anesthesia care unit with the epidural in place. Postoperative Considerations The priorities of care in the post anesthesia care unit are to first assess their ABCs: airway, breathing, and circulation. It is also necessary to check vital signs, oxygen saturation, and to monitor her heart. The nurse should also assess the patients urinary output. It is also important to assess for any signs or symptoms of hemorrhage/bleeding. If there were to be any excessive bleeding internally or externally, vital signs would show abnormalities. Specifically with a hysterectomy it is important to assess abdomen dressings for any bleeding for the first 8 hours after surgery (Lewis et al, 2007). Following these priorities would be your assessment of pain. In PACU, the patient was positioned supine. Immediately when transferred into the PACU, the nurse assessed her vital signs and hooked her up to a monitor that would automatically take them every 10 minutes. The nurse also hooked her up to telemetry and assessed her pain right away. The patient denied any pain and just stated she was tired. Before the patient is allowed to transfer onto a surgical unit or is discharged, there are five components that are assessed. The patient’s vital signs need to be stable, patient must be alert and responsive and is able to communicate any needs, patient’s pain should be at either a 2 or 3 on a scale of 1 9 Running Head: OPERATING ROOM REPORT to 10, patient shows no respiratory depression, and must have a temperature within the normal ranges, at least above 36 degrees Celsius. Accompanying a surgery, there are always complications that the patient is at risk for. With a hysterectomy, one large complication is a ureter ligation. Therefore it is important to closely monitor urinary output and make sure there is no urinary retention (Lewis et al, 2007). This is also why before they close the patient up after the uterus is removed, dye is injected in the patient to make sure the ureters are working properly. Another complication is deep vein thrombosis. According to Lewis etal., (2007), “it is important to frequently change positions, avoid the high Fowler position, and avoid pressure under the knees to minimize stasis and pooling of blood” (p. 1406). In order to keep the patient circulation moving, it is important to encourage them to do frequent leg exercises. Lastly, the patient could experience infection as a postoperative complication (Lewis et al, 2007). After a hysterectomy, infection can occur in the incision, the vagina, and bladder or inside the abdomen. Very rarely, infections can progress to an abscess, which is collection of bacteria and pus that must be drained. Based on this patient’s surgery, there are specific discharge instructions that the patient needs to follow. Lewis et al. (2007), indicates that “discharge teaching includes preparing the patient for what to expect following surgery, for example she will not be able to menstruate” (p.1406). Physical restrictions must be limited, but only for a short time. This includes no heavy lifting for 2 months and any activities that may increase pelvic congestions such as dancing and fast walking (Lewis et al, 2007). Also intercourse should be avoided until the wound is healed (Lewis et al, 2007). Some activities can help both physically and mentally, such as swimming (Lewis et al, 2007). Also wearing a girdle can enhance the patients comfort (Lewis et al, 2007). Once the patient is completely healed, these above activities can be resumed. Conclusion The perioperative period is a stressful time for both the patient and family. Effective nursing care during the preoperative, intraoperative, and postoperative periods can help make 10 Running Head: OPERATING ROOM REPORT this time period go by quickly and smoothly and lead to a speedy patient recovery. Operating room nurses, PACU nurses, and unit nurses all play significant roles in the process of providing patient-centered care. By working collaboratively with the surgical team and other providers involved in the patient’s recovery process, the nurse is able to ensure the best possible care while reducing complications. 11 Running Head: OPERATING ROOM REPORT References Deglin, J. H., & Vallerand, A. H. (2009). Davis’s drug guide for nurses. Philadelphia, PA: F. A. Davis Company. Lewis, S. L., Heitkemper, M. M., Dirksen, S. R., O’Brien, P. G. & Boucher, L. (2007). Medical-surgical nursing: Assessment and management of clinical problems. St. Louis, MI: Mosby. The Federal Government Source for Women’s Health information. Hysterectomy. Retrieved October 23, 2010, from http://www.womenshealth.gov/faq/hysterectomy.cfm#top