The oedematous patient
advertisement

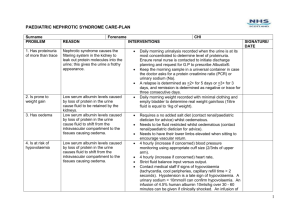
The oedematous patient Oedema is a collection of fluid in the interstitial tissue. Commonly oedema will collect in the legs as the fluid sinks to the lowest points in the body. Other sites fluid will collect are the pleural cavity (pleural effusion), the peritoneum (ascites) and the sacrum. Though fluid can accumulate anywhere in the body. To decide on the cause of the oedema and decide on treatment we must examine the patient, take a good history and investigate appropriately. Firstly look at the distribution of the oedema and does it pit when you push on it? The common causes of gross oedema of both legs and other sites are: Heart failure Renal failure Nephrotic syndrome Liver failure Protein malnutrition (not usually gross oedema) The common cause of single leg oedema which pits: Deep vein thrombosis The common causes of non-pitting single leg oedema: Lymphatic filariasis Radiotherapy Second take a full history This would be to suggest the likely cause. Has the patient any chest pain? Has the patient been short of breath? Have they got short of breath whilst walking? Do they wake up short of breath at night or need to sleep sat up to avoid being short of breath? These symptoms suggest heart failure. Is the urine out put ok? Is there any blood in the urine? These symptoms suggest renal failure. Do they have a history of drinking excess alcohol? Have they had any jaundice? These symptoms suggest liver failure. Deep vein thrombosis presents with a single leg swelling and aching. Often after or during pregnancy, surgery or spending a prolonged time in the same position (long bus rides). Provided by T. Whitfield 2012 Lymphatic filiariasis will occur gradually over time in endemic areas. Investigations for oedema Six tests should be done on bilateral oedematous patients: U+E Liver function tests Abdominal ultrasound Cardiac ultrasound Urinalysis and dipstick Chest x-ray U+E will highlight any renal failure; liver function tests will demonstrate any liver damage and low albumin. Low albumin could be a result of liver damage or chronic disease, albumin may also be lost through the kidney in nephrotic syndrome. Abdominal ultrasound will look at the kidneys and liver to demonstrate and cirrhosis or fattiness of the liver or shrinkage of the kidneys in renal failure. Cardiac ultrasound will look at the contractility of the heart and assess for heart failure. Urinalysis will demonstrate any protein lost in nephrotic syndrome (protein ++ on dipstick) and any blood or casts seen in glomerulonephritis. Nephrotic syndrome is a triad of oedema, low albumin and proteinuria. Chest x-ray will show any pulmonary oedema which is present in congestive cardiac failure and severe renal failure and nephrotic syndrome. Single oedematous legs should undergo ultrasound scanning to rule out any deep vein thrombosis. The history examination and investigations can be fit together to reach a diagnosis and treatment plan Provided by T. Whitfield 2012