File
advertisement

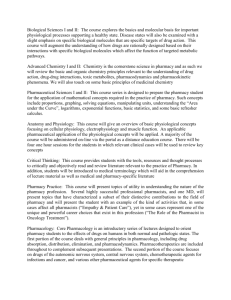
HYPOADRENOCORTICISM The Great Pretender Sarra Borne UID: 000493586 VETE 405: Pharmacology and Pharmacy Sarra Borne VETE 405: Pharmacology and Pharmacy UID: 000493586 November 30, 2013 Assignment: FINAL EXAM CASE STUDY Hypoadrenocorticism the Great Pretender Finnegan is a 9 year-old, normally 77- 79 lb, MN, Labradoodle who was initially referred to the internal medicine department of Veterinary Specialists of North Texas (VSNT) for increased renal values, and hyperphosphatemia. Finnegan was originally from the Washington D.C. area, and had only moved to Texas recently. Shortly after his arrival in the Dallas area, he had an episode of hind end collapse while going upstairs. This was his first such episode. His owners took him to the emergency clinic where he was examined and diagnosed with lower back pain and neuritis. At that time Finnegan was placed on Rimadyl ® (carprofen) at a dose of 75 mg PO q 24h (twice daily). The following day October 23rd 2013, Finnegan had another episode of apparent hind end weakness, so his owners took him to a local day practice. While there he was sedated and radiographs of his spine, shoulders, pelvis and coxofemoral joints were done. The cervical spine was overall normal, with no signs of degeneration or collapse. The lumbar spine, pelvis and coxofemoral joints were all within normal limits. Radiographically his shoulders showed the formation of osteophytes (bone spurs), and joint mice (small, loose pieces of bone in the synovial space) bilaterally on the caudal points of the humerus and his scapular rim showed some remodeling. He was assessed to have detectable pain in the right shoulder region, and osteoarthritis bilaterally, with the left being greater than the right. Osteoarthritis, also known as degenerative joint disease is a chronic degenerative disease that affects one or more joints in the body. It is caused by a deterioration of joint cartilage. Cartilage is a smooth, resilient tissue that lines the joints, allowing nearly frictionless joint movement and providing shock absorption. The deterioration of cartilage leads to increased 1 Sarra Borne VETE 405: Pharmacology and Pharmacy UID: 000493586 November 30, 2013 Assignment: FINAL EXAM CASE STUDY Hypoadrenocorticism the Great Pretender friction and inflammation of the joints. This erodes the bone and can cause formation of new bone, called osteophyte (bone spur) formation, which interferes with normal movement and can cause pain. (Lennon & Marcellin-Little, 2005) Figure 1: The x-ray on the left is an abnormal glenohumeral or shoulder joint. Image on the right is a normal glenohumeral joint. (Fairfield Veterinary Centre, n.d.) Finnegan’s owners were instructed to continue the Rimadyl ® as previously prescribed, and to return if there was no improvement or if there was another flare up of symptoms. On October 24th, Finnegan returned to the day practice with a complaint of vomiting, lethargy and inappetence. Finnegan was mildly dehydrated as evidenced by a decreased skin turgor and slightly tacky mucous membranes. His rectal temperature (T) was 99.4 and his weight was 68 lb. At this time a complete blood count and serum chemistry panel were run. The CBC was within normal limits other than a few changes related to dehydration, the serum 2 Sarra Borne VETE 405: Pharmacology and Pharmacy UID: 000493586 November 30, 2013 Assignment: FINAL EXAM CASE STUDY Hypoadrenocorticism the Great Pretender chemistry panel showed signs of moderate to marked azotemia, hyperphosphatemia, and a slight increase in plasma proteins. Blood values on 10/24/2013 from the day practice Normal Range (Heska) 103/ul WBC 13.0 6.0 -17.0 HCT 55.7 37-55 % RBC 8.94 5.50 – 8.50 106/ul BUN 127.7 9 – 29 mg/dl CREA 3.8 0.4 – 1.4 mg/dl Phos 13.7 1.9 – 5.0 mg/dl TP 7.9 5.5 – 7.6 g/dl Albumin 4.0 2.5 – 4.0 g/dl Globulin 3.9 2.0 – 3.6 g/dl ALT 87 0 – 120 U/L ALP 44 0 – 140 U/L GGT 15 0 – 14 U/L K 8.1 3.8 – 5.3 mEq/L Na 133 141 – 152 mEq/L Cl 108 102 – 120 mEq/L The assessment was renal insufficiency of undetermined cause. The differential included occult infection, leptospirosis, toxin exposure or neoplasia. At this point, Finnegan was referred to VSNT for monitored overnight hospitalization with intravenous fluids, and an ultrasound examination of the abdomen. The referring veterinarian was concerned that Finnegan might 3 Sarra Borne VETE 405: Pharmacology and Pharmacy UID: 000493586 November 30, 2013 Assignment: FINAL EXAM CASE STUDY Hypoadrenocorticism the Great Pretender have leptospirosis. The referring veterinarian sent leptospirosis titers to a reference lab, and they were not available at the time of his initial exam with the internists at VSNT. All seven of the tested serovars eventually came back negative effectively eliminating infection with leptospirosis as part of the differential. On Finnegan’s arrival at VSNT a complete history was taken. There was no history of toxic exposure, and no travel history other than the family move from the East Coast. The owners noted that Finnegan is a couch potato indoor dog. The owners commented that Finnegan had not recovered well from the anesthetic event the previous day, and was lethargic, had vomited several times, and wouldn’t eat. On physical examination it was noted that Finnegan was bright and alert. He had a rectal temperature (T) of 98.6 F, heart rate (HR) 132 bpm, respiratory rate (RR) 36 bpm, and weighed 70.4 lb on our scale. The abdominal palpation elicited discomfort on palpation of the kidney area. An abdominal ultrasound was done where it was discovered that Finnegan had a normal left kidney, and an absent right kidney. The radiologist had the following comments: Absent right kidney. Considerations are given to renal agenesis (one or both fetal kidneys fail to develop) or possibly a severe renal hypoplasia (an abnormally small kidney that has a reduced number of or smaller nephrons) resulting in unrecognizable renal tissue. The mild pelvic renal dilation on the left could be due to mild pyelonephritis (a urinary tract infection affecting the kidneys), renal insufficiency or fluid therapy. Otherwise a sonographically normal abdomen. A radiographic or CT intravenous pyelogram could be considered to evaluate the expected location of the right kidney. The ultrasound images are of Finnegan’s left kidney, and the area where his right kidney should be. 4 Sarra Borne VETE 405: Pharmacology and Pharmacy UID: 000493586 November 30, 2013 Assignment: FINAL EXAM CASE STUDY Hypoadrenocorticism the Great Pretender 5 Sarra Borne VETE 405: Pharmacology and Pharmacy UID: 000493586 November 30, 2013 Assignment: FINAL EXAM CASE STUDY Hypoadrenocorticism the Great Pretender A urinalysis via cystocentesis demonstrated the following values: Appearance Clear Color Dark Yellow Specific Gravity 1.076 Bacteria, WBC, Casts, Crystals, Epithelial None Seen Cells pH 6.5 RBC Occasional Finnegan was admitted to the hospital for aggressive fluid diuresis. He was prescribed ampicillin at 22 mg/kg IV q 6 h to treat for the potential leptospirosis. Finnegan was maintained in the quarantine area, and the staff was instructed to treat him as potentially infectious. Finnegan did well overnight, and the azotemia was almost completely resolved by the following morning. 10/25/13 6 AM Normal (Catalyst Analyzer) BUN 6am 33 7-27 mg/dl CREA 1.4 0.5 – 1.8 mg/dl Phos 4.5 2.5 – 6.8 mg/dl TP 6.3 5.2 – 8.2 % Globulin 3.2 2.5 – 4.5 g/dl Albumin 3.1 2.3 – 4.0 g/dl T. Bili 0.2 0.0 – 0.9 mg/dl Na 143 144 – 160 mmol/L K 7.6 3.5 – 5.8 mmol/L Cl 114 109 – 122 mmol/L 6 Sarra Borne VETE 405: Pharmacology and Pharmacy UID: 000493586 November 30, 2013 Assignment: FINAL EXAM CASE STUDY Hypoadrenocorticism the Great Pretender The fluid rate was decreased throughout the day, and his BUN remained within normal limits. 10/25/13 3 PM Normal BUN 24 7-27 mg/dl Na 144 144 – 160 mmol/L K 6.8 3.5 – 5.8 mmol/L Cl 113 109 – 122 mmol/L He was released that afternoon on oral doxycycline at 5 mg/kg q 12h, pending the leptospirosis results. It was recommended that Finnegan be fed a low protein diet such as Hill’s Prescription k/d or Purina Veterinary Diet NF, and that he be allowed free access to water. A recheck was scheduled with his primary vet for the following week. On 10/28/2013 Finnegan had another episode of collapse and was taken to the emergency clinic. His vital signs were 71.8 lb, rectal temperature 100.5 F, heart rate 76 bpm, respiratory rate 28 bpm. Alert. A CBC and serum chemistry were run, and the results showed a mild azotemia, hyperphosphatemia, hyperkalemia, hyponatremia, and a mildly increased hematocrit. 10/28/2013 9:25 PM Normal (Heska analyzer) HCT 57.5 37 – 55% BUN 63.1 9.0 – 29.0 mg/dl CREA 2.2 0.4 – 1.4 ,g/dl Phos 6.0 1.9 – 5.0 mg/dl Na 134 3.8 – 5.3 mEq/L K 8.5 141 – 152 mEq/L CL 108 102 – 120 mEq/L 7 Sarra Borne VETE 405: Pharmacology and Pharmacy UID: 000493586 November 30, 2013 Assignment: FINAL EXAM CASE STUDY Hypoadrenocorticism the Great Pretender Finnegan was hospitalized overnight on intravenous fluids, and referred back to VSNT for follow-up in the morning. A cardiac arrhythmia was noted by the emergency clinic possibly related to the elevated potassium. The differential diagnosis was still acute renal failure, leptospirosis, or other renal disease. On the morning of 10/29/13 Finnegan transferred back to VSNT for further care. His vital signs were 70.7 lb, rectal temperature 101.3, HR 90, RR panting. His owners related the following: “After coming home on 10/25 and sleeping for most of the day, he was steadily improving, ate some canned dog food. The following day he was more alert and ate hungrily and drank water, more like himself. Yesterday 10/28 Finny wanted to chase his ball, we went for a walk and he was himself, ate and drank normally, had a normal bowel movement, on evening walk around 8pm he would not get up so we took him next door (emergency hospital). It was again noted that Finnegan had an irregular heartbeat, so the doctor ordered an ECG. The results were consistent with hyperkalemia. Tall, peaked T-waves, shortened QT interval, and a depressed ST segment. This particular pattern was the result of atrial standstill which is the lack of atrial activity resulting from a failure of atrial depolarization. The ventricles still function normally. This can be caused by electrolyte abnormalities especially hyperkalemia (which can develop secondary to a number of conditions including Addison’s disease, oliguric renal failure and urethral obstruction), cardiomyopathy, muscular dystrophy and drug toxicity. (WikiVet, 2013) 8 Sarra Borne VETE 405: Pharmacology and Pharmacy UID: 000493586 November 30, 2013 Assignment: FINAL EXAM CASE STUDY Hypoadrenocorticism the Great Pretender The atrial standstill and the hyperkalemia, and the hyponatremia, plus the faxed copy of the negative leptospirosis titers were highly suspicious for hypoadrenocorticism or Addison’s disease. An ACTH stimulation test was ordered. A baseline serum cortisol sample was drawn, a dose of cosyntropin at 5mcg/kg was given IV and a post ACTH serum cortisol sample was drawn an hour later. The results were conclusive. PRE ACTH CORTISOL <0.2 ug/dl POST ACTH CORTISOL <0.2 ug/dl ACTH reference range: <2 Post-ACTH cortisol consistent with hypoadrenocorticism. Finnegan was again hospitalized overnight and given a loading dose of dexamethasone sodium phosphate at 0.15 mg/kg IV, and then a second dose 12 hours later at 0.075 mg/kg IV. He was maintained on 5% Dextrose in 0.9 % NaCl intravenous fluids, and did remarkably well overnight. The following day he was treated with the mineralocorticoid Percorten-V ® (DOCP or desoxycorticosterone pivalate) at 2.2 mg/kg IM, which is to be repeated every 25 days. DOCP is a long-acting mineralocorticoid agent which is indicated for the parenteral treatment of adrenocortical insufficiency in dogs (Plumb, 2011). That afternoon Finnegan was released with a prescription for Prednisone 30 mg PO q 24 hr for 3 day, then 20 mg PO q 24 hr for 7 day, then 10 mg PO q 24 hr until otherwise directed. The owners were instructed to continue the low protein diet, and return in 10 days for a recheck examination. They were also given several handouts on Addison’s disease. 9 Sarra Borne VETE 405: Pharmacology and Pharmacy UID: 000493586 November 30, 2013 Assignment: FINAL EXAM CASE STUDY Hypoadrenocorticism the Great Pretender We saw Finnegan back on 11/11/13 and he looked remarkable. His energy and appetite were back. He had no further episodes of collapse, and his blood work was all within normal limits. A recheck was scheduled for two weeks for another DOCP injection and electrolytes. 11/11/13 Normal (Catalyst) BUN 22 7-27 mg/dl Creat 1.3 0.5-1.8 mg/dl Phos 3.7 2.5-6.8 mg/dl Na 154 144-160 mmol/L K 3.9 3.5-5.8 mmol/L Cl 118 109-122 mmol/L The owners had some concerns about the cost involved in the DOCP injections, as Finnegan is a rather large dog, and DOCP is not inexpensive. The discussed it with the internist and the decision was made to switch to fludrocortisone (Florinef ®) which is an oral mineralocorticoid at a dose of 0.01 mg/kg q 12 hr. Finnegan’s dose came out to 0.3 mg. Commercially available fludrocortisone is only available in 0.1 mg tablets, so his prescription was called into a compounding pharmacy. Fludrocortisone has some glucocorticoid activity as well as mineralocorticoid, so it may have more side effects than DOCP. These may include polyuria, polydipsia, polyphagia, and poor skin and coat. If Finnegan receives an overdose it could lead to hypotension, hypernatremia, edema, and hypokalemia. Monitoring is crucial, especially during his first few months of therapy (Brooks, 2012). 10 Sarra Borne VETE 405: Pharmacology and Pharmacy UID: 000493586 November 30, 2013 Assignment: FINAL EXAM CASE STUDY Hypoadrenocorticism the Great Pretender Finnegan returned for another follow-up visit on 11/26/2013. His owners are very pleased with his progress. He is eating and drinking normally, has a normal activity level, and takes his medications well. Their only complaint is that Finnegan is having some soft stool with occasional mucus, but no blood. His vital signs were good. T 99.1 F, HR 140, RR 50. He is back to his normal weight of 76.9 lb. An electrolyte panel was ordered and all values were within normal limits. 11/26/13 Normal (Catalyst) Na 159 144-160 mmol/L K 3.6 3.5-5.8 mmol/L Cl 44 109-122 mmol/L A rectal exam was done and it was normal. There were no parasites found on a fecal flotation. It was suggested that the owners try adding some fiber to Finnegan’s diet, which currently consists mostly of canned Hill’s Prescription Diet k/d. Some methods of doing this are adding green beans, carrots and/or canned pumpkin. Also ¾ tsp. of Benefiber or Metamucil may be of benefit. Finnegan’s next recheck is scheduled for a month. His fludrocortisone is to be refilled as needed. Hypoadrenocorticism or Addison’s disease is a deficiency of adrenocortical hormones that is most commonly seen in young to middle-aged dogs. It may be familial in Standard Poodles, so Finnegan may have inherited the genetic disposition from his Poodle ancestors. Clinical signs of Addison’s disease are often indistinct. They may be acute or chronic, appear episodic for weeks or even months and intensify in stressful situations (Labor fur Klinische Diagnostik, 2009). This is one of the reasons that Addison’s disease is known as “the great pretender”, it has the ability to mimic other common canine diseases. The 11 Sarra Borne VETE 405: Pharmacology and Pharmacy UID: 000493586 November 30, 2013 Assignment: FINAL EXAM CASE STUDY Hypoadrenocorticism the Great Pretender differential diagnosis list is long and includes primary GI disease (especially infection with Trichuris vulpis or whipworm), renal failure, liver failure, uroabdomen, pleural effusion, acute pancreatitis, toxin ingestion, leptospirosis, neurologic disease and many others. History, physical exam findings, and other diagnostics should help whittle down this list. pathognomonic clinical signs for hypoadrenocorticism and There are no naturally occurring hypoadrenocorticism is an uncommon canine disease with estimates of its incidence ranging from 0.36% to 0.5 % (Klein & Peterson, 2010). Naturally occurring primary adrenocortical failure occurs from atrophy or destruction of all three adrenal cortical layers, which results in inadequate secretion of both mineralocorticoids and glucocorticoids (Kintzer & Peterson, 1997). Immune mediated destruction of the adrenal cortex appears to cause this form of primary hypoadrenocorticism, and is the most common reason for primary hypoadrenocorticism in humans (Feldman & Nelson, 2004). Hyperkalemia, hyponatremia, hypochloremia, and decreased sodium to potassium ratios represent the classic electrolyte changes in Addisonian dogs, and hypoadrenocorticism should be on the differential list anytime this pattern of electrolyte imbalance is seen. A definitive diagnosis of Addison’s disease can be made with the ACTH stimulation test. Dogs with Addison’s disease do not possess adequate reserves of cortisol to adequately respond. The prognosis is fairly good. Finnegan will require lifelong mineralocorticoid and glucocorticoid supplementation. His serum electrolytes will need to be monitored on a regular basis, every few weeks until he stabilizes, and then quarterly. However, with drug therapy he can return to being a clinically normal and healthy animal with normal blood parameters. A study evaluating long-term treatment of 205 dogs with hypoadrenocorticism (1979-1993) 12 Sarra Borne VETE 405: Pharmacology and Pharmacy UID: 000493586 November 30, 2013 Assignment: FINAL EXAM CASE STUDY Hypoadrenocorticism the Great Pretender reported that there was a good to excellent response to treatment in more than 80% of the dogs, and a fair response tin 12.5% (Kintzer & Peterson, 1997) The median survival time for dogs in this study was 4.7 years and many of the dogs were still alive at the end of the study period. There was no difference in survival time between dogs treated with fludrocortisone versus DOCP. Of the 124 dogs that died, 120 expired for reasons unrelated to hypoadrenocorticism (Kintzer & Peterson, 1997) 13 Sarra Borne VETE 405: Pharmacology and Pharmacy UID: 000493586 November 30, 2013 Assignment: FINAL EXAM CASE STUDY Hypoadrenocorticism the Great Pretender References Brooks, W. (2012, March 6). Fludrocortisone acetate. Retrieved from VeterinaryPartner.com: http://www.veterinarypartner.com/Content.plx?A=536 Feldman, E., & Nelson, R. (2004). Canine and feline endocrinology and reproduction (3 ed.). St. Louis, Missouri: WB Saunders. Kintzer P.P., P. M. (1997, March). Primary and secondary canine hypoadrenocorticism. Veterinary Clinics of North America Small Animal Practice, 27(2), 349-357. Kintzer, P., & Peterson, M. (1997, Mar-Apr). Treatment and long-term follow-up of 205 dogs with hypoadrenocorticism. Journal of Veterinary Internal Medicine, 11(2), 43-49. Klein, S., & Peterson, M. (2010, January). Canine hypoadrenocorticism: Part 1. The Canadian Veterinary Journal, 51(1), 63-69. Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2797351/ Labor fur Klinische Diagnostik. (2009, June). Addison's disease in dogs: What do lab results tell us. Retrieved from Laboklin Aktuell: http://www.laboklin.de/pdf/en/aktuell/lab_akt_0906_en.pdf Lennon, E., & Marcellin-Little, D. (2005). Canine Osteoarthritis. Retrieved from Arthritis M.D.: http://www.arthritismd.com/canine-osteoarthritis.html Normal Shoulder Joint. Fairfield Veterinary Centre, Leicestershire, UK. Retrieved from http://www.fairfieldvets.co.uk/ic/dog/erin-1.htm Plumb, D. (2011). Plumb's Veterinary Drug Handbook (Vol. 7). Ames, Iowa: Wiley-Blackwell. WikiVet. (2013, October 15). Atrial Standstill. Retrieved from http://en.wikivet.net/Atrial_Standstill 14